
Abstract
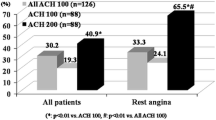
According to the Japanese Circulation Society guideline of vasospastic angina, incremental doses of acetylcholine (ACh) are prescribed for coronary spasm provocation: 20 and 50 μg for the right coronary artery (RCA), and 20, 50 and 100 μg for the left coronary artery (LCA). However, provocation by low doses of ACh in patients with low vasoreactivity may be less needed, and the requirement of 50 μg of ACh for the LCA in these patients has not been evaluated. In the present study, patients who underwent ACh provocation test for both the RCA and LCA were included. The positive diagnosis of intracoronary ACh provocation test was defined as total or subtotal coronary artery narrowing (i.e., angiographic coronary artery spasm) accompanied by chest pain and/or ischemic electrocardiographic changes. Coronary artery constriction was visually evaluated and defined as coronary artery diameter reduction <25 or 25–90% in patients without angiographic coronary artery spasm by 20 µg of ACh in the LCA. There were 33 out of 249 patients (13%) with LCA spasm by 20 µg of ACh. In subjects without LCA spasm by 20 µg of ACh, patients with coronary constriction <25% (n = 101) by 20 µg of ACh in the LCA rarely showed coronary artery spasm induced by 50 μg of ACh in the LCA, in comparison to those with coronary constriction 25–90% (n = 115) (2.6 vs. 32.7%, p < 0.001). None of the patients with coronary constriction <25% by 20 µg of ACh in the LCA had cardiac complications associated with administration of ACh. In conclusion, omission of 50 µg of ACh in the LCA may be possible when there is little coronary artery constriction by 20 µg of ACh in the LCA during provocation test, leading to less contrast and shortens overall procedure time.

Similar content being viewed by others

References
Takagi Y, Yasuda S, Takahashi J, Takeda M, Nakayama M, Ito K, Hirose M, Wakayama Y, Fukuda K, Shimokawa H (2009) Importance of dual induction tests for coronary vasospasm and ventricular fibrillation in patients surviving out-of-hospital cardiac arrest. Circ J 73:767–769
Ong P, Athanasiadis A, Borgulya G, Voehringer M, Sechtem U (2011) 3-year follow-up of patients with coronary artery spasm as cause of acute coronary syndrome: the CASPAR (coronary artery spasm in patients with acute coronary syndrome) study follow-up. J Am Coll Cardiol 57:147–152
Okumura K, Yasue H, Matsuyama K, Goto K, Miyagi H, Ogawa H, Matsuyama K (1988) Sensitivity and specificity of intracoronary injection of acetylcholine for the induction of coronary artery spasm. J Am Coll Cardiol 12:883–888
Sueda S, Ochi N, Kawada H, Matsuda S, Hayashi Y, Tsuruoka T, Uraoka T (1999) Frequency of provoked coronary vasospasm in patients undergoing coronary arteriography with spasm provocation test of acetylcholine. Am J Cardiol 83:1186–1190
Yasue H, Horio Y, Nakamura N, Fujii H, Imoto N, Sonoda R, Kugiyama K, Obata K, Morikami Y, Kimura T (1986) Induction of coronary artery spasm by acetylcholine in patients with variant angina: possible role of the parasympathetic nervous system in the pathogenesis of coronary artery spasm. Circulation 74:955–963
Sueda S, Izoe Y, Kohno H, Fukuda H, Uraoka T (2005) Need for documentation of guidelines for coronary artery spasm: an investigation by questionnaire in Japan. Circ J 69:1333–1337
Ong P, Athanasiadis A, Borgulya G, Mahrholdt H, Kaski JC, Sechtem U (2012) High prevalence of a pathological response to acetylcholine testing in patients with stable angina pectoris and unobstructed coronary arteries. The ACOVA Study (Abnormal COronary VAsomotion in patients with stable angina and unobstructed coronary arteries). J Am Coll Cardiol 59:655–662
Sueda S, Kohno H, Miyoshi T, Sakaue T, Sasaki Y, Habara H (2015) Maximal acetylcholine dose of 200 μg into the left coronary artery as a spasm provocation test: comparison with 100 μg of acetylcholine. Heart Vessels 30:771–778
JCS Joint Working Group (2014) Guidelines for diagnosis and treatment of patients with vasospastic angina (Coronary Spastic Angina) (JCS 2013). Circ J 78:2779–2801
Saito Y, Kitahara H, Shoji T, Tokimasa S, Nakayama T, Sugimoto K, Fujimoto Y, Kobayashi Y (2016) Intracoronary acetylcholine provocation testing—omission of the 20-µg dose is feasible in patients without coronary artery spasm in the other coronary artery. Circ J 80:1820–1823
Sueda S, Kohno H (2016) Overview of complications during pharmacological spasm provocation tests. J Cardiol 68:1–6
Sueda S, Miyoshi T, Sasaki Y, Sakaue T, Habara H, Kohno H (2016) Safety and optimal protocol of provocation test for diagnosis of multivessel coronary spasm. Heart Vessels 31:137–142
Sueda S, Kohno H, Ochi T, Uraoka T (2015) Overview of the acetylcholine spasm provocation test. Clin Cardiol 38:430–438
Kitahara H, Kobayashi Y, Iwata Y, Fujimoto Y, Komuro I (2011) Effect of pioglitazone on endothelial dysfunction after sirolimus-eluting stent implantation. Am J Cardiol 108:214–219
Aoki Y, Ishikawa K, Miura K, Sugimoto K, Nakayama T, Fujimoto Y, Kobayashi Y (2016) Protective effect of angiotensin II receptor blocker and calcium channel blocker on endothelial vasomotor function after everolimus-eluting stent implantation. J Cardiol 67:236–240
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict and interest
None.
Rights and permissions
About this article

Cite this article
Saito, Y., Kitahara, H., Shoji, T. et al. Feasibility of omitting provocation test with 50 μg of acetylcholine in left coronary artery. Heart Vessels 32, 685–689 (2017). https://doi.org/10.1007/s00380-016-0926-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00380-016-0926-7