
Abstract
Objectives
Previous analyses of the impact of median lobe presence on Greenlight photoselective vaporization of the prostate (PVP) outcomes were limited by their small sample size and the ability to adjust for important confounders. As such, we sought to investigate the impact of prostate median lobe presence on the operative outcomes of 180 W XPS GreenLight PVP using a large international database.
Methods
Data were obtained from the Global GreenLight Group (GGG) database which pools data of eight high-volume, experienced surgeons, from a total of seven international centers. All men with established benign prostatic hyperplasia who underwent GreenLight PVP using the XPS-180 W system between 2011 and 2019 were eligible for the study. Patients were assigned to two groups based on presence or absence of median lobes. Analyses were adjusted for patient age, prostate volume, body mass index, and American Society of Anesthesia (ASA) score.
Results
A total of 1650 men met the inclusion criteria. A median lobe was identified in 621 (37.6%) patients. Baseline prostate volume, patient age, and ASA score varied considerably between the two groups. In adjusted analyses, the operative and lasing time of patients with median lobes was 6.72 (95% CI 3.22–10.23; p < 0.01) minutes and 2.90 (95% CI 1.02–4.78; p < 0.01) minutes longer than the control group. Men with median lobes had similar postoperative functional outcomes to those without a median lobe except for a 1.59-point greater drop in the 12-month IPSS score compared to baseline (95% CI 0.11–3.08; p = 0.04) in the median lobe group, and a decrease in PVR after 6 months which was 46.51 ml (95% CI 4.65–88.36; p = 0.03) greater in patients with median lobes compared to men without median lobes.
Conclusions
Our findings suggest that the presence of a median lobe has no clinically significant impact on procedural or postoperative outcomes for patients undergoing Greenlight PVP using the XPS-180 W system.
Similar content being viewed by others

Introduction
GreenLight photoselective vaporization of the prostate (PVP) is a safe and effective treatment option for benign prostatic hyperplasia (BPH) in small-to-moderate-sized prostates (30–80 cc) [1,2,3,4]. In the context of larger prostates (> 100 cc), it has been shown to be an acceptable alternative to available modalities [5,6,7], but has been associated with longer operative time, more bleeding, and rising retreatment rates after 3 years, amongst other limitations [7,8,9].
It is challenging to disentangle the effect of larger prostate volumes from the effect of the median lobe on these outcomes, as both are closely related. Many men presenting with greater prostate volumes often present with a median lobe, also known as an intravesical prostatic protrusion (IPP) [10, 11]. The median lobe may complicate the surgical procedure, making it more difficult to safely achieve adequate tissue removal [12,13,14]. Conditions such as a high bladder neck, bladder neck bleeding, and/or IPP obstructing the visualization of the ureteral orifices can lead to incomplete vaporization and less favourable functional outcomes [15]. These difficulties have led some to investigate whether a combination of vaporization-resection would be beneficial over vaporization alone in patients with median lobes [16].
However, previous studies investigating the impact of the median lobe on BPH surgery outcomes have been limited in their ability to adjust for prostate size due to a small sample sizes [12, 16,17,18,19]. Despite it being commonly accepted that prostate configuration has little effect on the efficiency of GreenLight laser PVP, there are no studies specifically studying the impact of a median lobe on outcomes of interest while adjusting for potential sources of confounding such as prostate volume. As such, we sought to evaluate the impact of median lobe presence on outcomes of GreenLight PVP while adjusting for prostate size, amongst other factors, using a large, international GreenLight PVP database.
Methods
Data source
Data were obtained from the Global GreenLight Group (GGG) database [20]. At the time of analysis, the database was composed of 3809 men with established BPH who underwent treatment using solely GreenLight PVP using the XPS-180 W system between 2011 and 2019, as performed by high-volume, experienced surgeons, at a total of seven centers in Canada, Mexico, Brazil, Argentina, Italy, France, and Germany. Patients requiring a hybrid procedure involving enucleation were not included in the database. Indications for surgery in each country were based on similar criteria established by the Canadian Urological Association, American Urological Association, and European Association of Urology guidelines on BPH surgical management [2, 21, 22].
Cohort exclusion criteria
We excluded patients with a previous history of transurethral resection of the prostate (TURP), a prostate size under 30 cc, missing median lobe information, known prostate cancer, previous pelvic radiation, or known neurological disorders. All other patients were included.
Definition of the exposure
A median lobe was identified during preoperative cystoscopy as a distinct intravesical protrusion and each patient was coded as either having a median lobe or not having a median lobe. No other median lobe measurement was available. All patients underwent a preoperative cystoscopy. The presence of a median lobe was also further confirmed on transrectal ultrasound (TRUS) (Fig. 1). Prostate size was measured with TRUS using the ellipsoid formula (height × width × length × π/6) [23].

Cystoscopy and ultrasound findings of a prostatic median lobe. a Cystoscopy findings with absence of a median lobe. b Cystoscopy findings demonstrating distinct intravesical median lobe protrusion. c Corresponding ultrasound image confirming the anatomy/configuration of intravesical prostatic protrusion
Study parameters
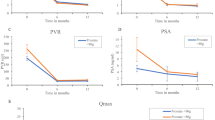
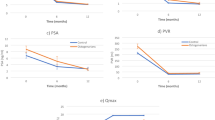
Patients completed the International Prostate Symptom Score (IPSS) questionnaire for lower urinary tract symptoms, including the 6-point quality of life (QoL) score questionnaire. Uroflowmetry was performed, as well as measurements of the post-void residual (PVR). Prostate-specific antigen (PSA) levels were determined in a standard laboratory blood assessment. Prostate size was measured using the TRUS approach. American Society of Anesthesiologists (ASA) score was used as an indicator for patients’ general health/fitness status. Operative time, postoperative hematuria rate, blood transfusion rate, hospital length of stay (LOS) and readmission rates were also documented. Questionnaires, uroflowmetry, PVR and laboratory tests were required at the postoperative visits at 6 and 12 months (Fig. 2).

One-year functional outcomes of Greenlight PVP based on presence of median lobe. a IPSS score, b QoL score, c PVR, d PSA, e Qmax
Covariates
Covariates included age, prostate size as measured via transrectal ultrasound (categorized as 30–80 cc, 80–150 cc, ≥ 150 cc in adjusted analyses), body mass index (BMI), and ASA score (categorized as 0, 1, 2, ≥ 3).
Statistical analysis
Means and standard deviations were reported for continuous variables. Categorical variables were presented as frequencies and proportions.
In unadjusted analyses comparing the outcomes of patients with median lobes to those of patients without median lobes, the two-sided t-test was used for continuous outcomes, the Pearson chi-square test for dichotomous outcomes, and the Wilcoxon rank-sum for the non-parametric outcome of hospital LOS. Unadjusted analyses were performed to provide a reference to compare our cohort to that of previous unadjusted analyses of smaller cohorts.
In adjusted analyses, multivariable linear regression models adjusting for the previous listed covariates were fitted to compare continuous outcomes between patients with and without median lobes. For dichotomous outcomes, multivariable logistic regression models adjusting for the covariates were used to estimate the odds of the outcome between both groups. For rare outcomes (transfusions and hematuria), we used Firth’s multivariable logistic regression, again adjusting for all covariates [24]. Hospital LOS was non-normally distributed and as such was log-transformed for adjusted regression analyses. However, all results are presented in non-log-transformed measures to facilitate interpretability.
Statistical analyses were performed using Stata version 14.0 (StataCorp, Texas, USA). Statistical significance was defined as a two-sided p < 0.05. Institutional review board approval was obtained prior to the conduct of this study.
Results
Baseline characteristics
A total of 1650 men met our inclusion criteria. Patients in the median lobe group were on average 1 year younger than patients without a median lobe (p = 0.04). A median lobe was identified in 621 (37.6%) patients. The prostate volume, measured by TRUS, was significantly larger in the median lobe group compared to the absent median lobe group (86.44 ml vs 78.30 ml, respectively; p < 0.01). ASA scores varied considerably between the two groups with favorable scores found in patients in the median lobe group (p < 0.01). IPSS scores were comparable in both groups (p = 0.08). Patients in both groups demonstrated peak urinary flow rates around 7 ml/s (p = 0.13). Additional patient baseline characteristics can be found in Table 1.
Unadjusted perioperative and functional outcomes
Operative time was longer in the median lobe group compared to the control group (76.17 min and 65.35 min, respectively, p < 0.01). The median lobe group also had a significantly longer lasing time (41.70 min vs 38.78 min, respectively, p < 0.01). No difference was appreciated for lasing energy (p = 0.93) or hospital LOS (p = 0.07). At both 6- and 12-month follow-up, mean maximum urinary flow rate (Qmax) improvements were significantly greater in patients with median lobes (an improvement of 13.0 ml/s vs. 11.75 ml/s at 6-months and 13.4 ml/s vs. 11.79 ml/s at 12 months for median lobe vs no median lobe group, respectively; p = 0.01 and p < 0.01, respectively). Additional unadjusted perioperative and functional outcomes can be found in Table 2 and Fig. 1.
Adjusted perioperative and functional outcomes
In analyses adjusting for age, BMI, ASA score, and prostate volume category, the operative time in the median lobe group was 6.72 (95% CI 3.22–10.23; p < 0.01) minutes longer than the control group. Patients with median lobes had 2.90 min longer lasing time (95% CI 1.02–4.78; p < 0.01). Comparable postoperative LOS was seen in both groups. There were no statistically significant differences for both transfusion rates [OR 0.42 (95% CI 0.02–10.44; p = 0.60)] and hematuria rates [OR 1.20 (95% CI 0.67–2.15; p = 0.53)]. Similarly, patients with a median lobe had comparable odds [OR 1.07 (95% CI 0.63–1.82; p = 0.796)] of being readmitted within 30 days.
IPSS changes at 6-month follow-up were not statistically different in the median group compared to the control group [+ 0.91 (95% CI − 0.33 to 2.14; p = 0.15)]. Comparatively, the IPSS drop after 12 months demonstrated a 1.59-point improvement (95% CI 0.11–3.08; p = 0.04) in the median lobe group. Changes in QoL scores in the median lobe group were similar to the control group at 6- and 12-month follow-up [+ 0.21 (95% CI − 0.09 to 0.51; p = 0.165) and 0.32-point improvement (95% CI − 0.01 to 0.66; p = 0.06), respectively]. The decrease in PVR after 6 months was 46.51 ml (95% CI 4.65–88.36; p = 0.03) greater in patients with median lobes compared to men without median lobes. However, the difference was non-significant at 12 months of follow-up [45.34 ml improvement (95% CI − 3.7 to 94.4 l; p = 0.07)]. Patients with median lobes had a similar Qmax to patients without median lobes at both 6- and 12-month follow-up [difference: − 0.03 (95% CI − 1.23 to 1.17; p = 0.23) and − 0.66 (95% CI − 1.74 to 0.42; p = 0.96), respectively].
Discussion
Larger prostate sizes are generally associated with more complications and worse outcomes compared to smaller glands [7,8,9]. Increasing prostatic volume is also associated with more complex anatomy, notably the presence of median lobes [10, 11]. They are thought to complicate surgery, particularly due to concerns of inadequate prostatic adenoma resection. However, previous studies comparing Greenlight PVP outcomes of patients with or without median lobes were limited by small sample sizes and could not adjust for prostate volume [15, 18, 19]. In our analysis of the GGG database adjusting for prostate volume categories and other factors, we found no significant differences in outcomes between patients with or without median lobes undergoing GreenLight PVP.
Patients presenting with LUTS and median lobe enlargement have been found to have decreased peak urinary flow rates and higher incidence of urinary retention when compared to patients with other prostatic configurations [19, 25]. Previous literature suggested that the presence of a median lobe may result in worse functional outcomes. Using a fluid structural interaction analysis approach using 3D models, Zheng et al. found that variations in prostate anatomy such as large IPPs lead to reduced flow efficiency [26]. In the clinical setting, the presence of a large median lobe has been found to be a predictor of trial without catheter failure [27]. Furthermore, studies have shown that greater length of IPP is associated with lower response to alpha-blockers and 5-alpha-reductase-inhibitors [28, 29]. This is believed to be secondary to the IPP of the enlarged median lobe creating a ball-valve mechanism with the opening of the bladder neck and/or causing abnormal bladder contraction with loss of the funnel effect of the bladder neck during voiding [15].
Men with median lobes undergoing GreenLight PVP using the 180 W XPS system had similar postoperative outcomes to those without a median lobe. Like Gu et al.’s findings, the operation time in our study was significantly longer in cases with a median lobe both in non-adjusted and adjusted analysis, although the absolute difference was small. This can likely be explained by a more extensive prostatic floor treatment as more time is required to vaporize the additional prostatic tissue of the enlarged median lobe. Zorn et al. described that patients with a median lobe will receive a second grooved incision at 7 o’clock prior to prostatic floor treatment [13]. Additionally, Kim et al. mention that a large protruding median lobe increases the difficulty of ureteral orifice identification [16]. Gu et al. studied the impact of median lobe presence on GreenLight PVP using the 120 W HPS [18]. In their study, the bilobed prostate group was compared to the trilobed group and was found to have a shorter lasing time and operation time. However, significant differences were present at baseline between the groups. Therefore, due to a lack of an adjusted analysis, it is impossible to appreciate the effect of median lobe on both perioperative and postoperative outcomes in their study.
In our study, there were no differences in safety outcomes in both groups. Patients in both groups had similar postoperative hospital LOS, hematuria rates, and rehospitalization rates, even after adjusting for age, prostate volume, BMI and ASA scores.
Adjusted 1-year functional outcomes in both groups were comparable except for statistically significant favorable outcomes in the median lobe group with regards to 6-month change in PVR and 12-month change in IPSS. Using GreenLight PVP 120 W HPS, Kim et al. noted a statistically significant difference in total IPSS and voiding IPSS sub-score in favor of the median lobe group at 1-month and 3-month follow-up, but not at 6-month follow-up [19]. This greater initial improvement is thought to be due to the different underlying mechanisms of obstruction between both groups. In patients without an obstructing median lobe, the cause of obstruction is predominantly due to increased intraluminal pressure of the prostatic urethra. In comparison, in patients with median lobes, the sudden elimination of the protruding intravesical mass may lead to a more rapid initial improvement of outlet obstruction [19].
We found a significant difference in Qmax change from baseline at 6- and 12-month follow-up in unadjusted analysis. However, the mean Qmax was similar between both groups at each follow-up period. Kim et al. also noted a statistically favourable change in Qmax from baseline at 6-month follow-up in their median lobe group compared to the control group [19]. However, in contrast to our findings, patients with median lobes in their study had a significantly lower preoperative Qmax compared to those without median lobes. Furthermore, after adjusting for covariates in our study, we no longer appreciated a difference in Qmax change from baseline in between the groups. These findings therefore support the hypothesis that the presence of a median lobe is not an independent predictor of the postoperative outcomes of GreenLight PVP.
The limitations of this study include its retrospective design and short follow-up period. The GGG database includes data of multiple high-volume international urological centers with experienced surgeons, which may not be representative of the lower-volume or more novice surgeons. The extent of median lobe IPP was not quantified as median lobe volume and anatomy were not collected. Although, previous studies suggest that there is no statistically significant correlation between degree of IPP and postoperative outcomes such as IPSS score, storage symptom score, voiding symptom score, QoL, Qmax and PVR [15].
Nevertheless, this is the first study which looks at the outcomes of GreenLight PVP in patients with median lobes while adjusting for confounding factors. The large sample size of our study allowed us to adjust for confounders, further isolating the impact of the median lobe on operative outcomes. Future research should examine the impact of median lobes on other modalities, namely enucleation which should be considered for patients presenting with a median lobe.
Conclusion
In a retrospective analysis of a large, international database of GreenLight PVP using the XPS-180 W system, we found no clinically significant differences in procedural or postoperative outcomes between patients with and without median lobes. Any differences previously observed in the literature may be due to low numbers limiting the ability to adjust for prostate size. Our findings support the hypothesis that GreenLight PVP is an effective modality for prostates with median lobes. Future studies will be required to determine the impact of median lobe presence on outcomes based on the dimensions of the median lobe.
References
Bachmann A, Tubaro A, Barber N et al (2014) 180-W XPSgreenlight laser vaporisation versus transurethral resection of the prostate for the treatment of benign prostatic obstruction: 6-month safety and efficacy results of a European multicentre randomised trial—The GOLIATH study. EurUrol 65:931–942. https://doi.org/10.1016/j.eururo.2013.10.040
Foster HE, Barry MJ, Dahm P et al (2019) Re: Surgical management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA Guideline. J Urol 203:1219. https://doi.org/10.1016/j.juro.2018.09.058
Brunken C, Seitz C, Woo HH (2015) A systematic review of experience of 180-W XPSGreenLight laser vaporisation of the prostate in 1640 men. BJU Int 116:531–537. https://doi.org/10.1111/bju.12955
Ghobrial FK, Shoma A, Elshal AM et al (2020) A randomized trial comparing bipolar transurethral vaporization of the prostate with GreenLight laser (xps-180watt) photoselective vaporization of the prostate for treatment of small to moderate benign prostatic obstruction: outcomes after 2 years. BJU Int 125:144–152. https://doi.org/10.1111/bju.14926
Hueber PA, Bienz MN, Valdivieso R et al (2015) Photoselective vaporization of the prostate for benign prostatic hyperplasia using the 180 watt system: multicenter study of the impact of prostate size on safety and outcomes. J Urol 194:462–469. https://doi.org/10.1016/j.juro.2015.03.113
Valdivieso R, Hueber PA, Meskawi M et al (2018) Multicentre international experience of 532-nm laser photoselective vaporization with GreenLightXPS in men with very large prostates. BJU Int 122:873–878. https://doi.org/10.1111/bju.14208
Stone BV, Chughtai B, Kaplan SA et al (2015) GreenLight laser for prostates over 100 ml: what is the evidence? CurrOpinUrol 26:28–34. https://doi.org/10.1097/MOU.0000000000000237
Meskawi M, Hueber PA, Valdivieso R et al (2019) Complications and functional outcomes of high-risk patient with cardiovascular disease on antithrombotic medication treated with the 532-nm-laser photo-vaporization GreenlightXPS-180 W for benign prostate hyperplasia. World J Urol 37:1671–1678. https://doi.org/10.1007/s00345-018-2560-8
Nguyen DD, Misraï V, Bach T et al (2020) Operative time comparison of aquablation, greenlightPVP, ThuLEP, GreenLEP, and HoLEP. World J Urol. https://doi.org/10.1007/s00345-020-03137-8
Audouin M, Girshovich A, Cussenot O, Renard-Penna R (2018) Typology of intravesical prostatic protrusions, or so-called median lobes, in middle-aged and older men. SurgRadiolAnat 40:389–393. https://doi.org/10.1007/s00276-018-1999-z
Lieber MM, Jacobson DJ, McGree ME et al (2009) Intravesical prostatic protrusion in men in Olmsted County, Minnesota. J Urol 182:2819–2824. https://doi.org/10.1016/j.juro.2009.08.086
Bodokh Y, Treacy PJ, Imbert de la Phalecque L, Durand M (2018) Does prostate median lobe really matter for GreenLightHPS laser photovaporization of the prostate. J Endourol Case Rep 4:169–172. https://doi.org/10.1089/cren.2018.0053
Zorn KC, Liberman D (2011) GreenLight180WXPSphotovaporization of the prostate: how I do it. Can J Urol 18:5918–5926
Law KW, Elterman DS, Cash H et al (2019) Anatomic GreenLight laser vaporization-incision technique for benign prostatic hyperplasia using the XPSLBO-180W system: how I do it. Can J Urol 26:9963–9972
Wee JH, Choi YS, Bae WJ et al (2012) Influence of intravesical prostatic protrusion on preoperative lower urinary tract symptoms and outcomes after 120 W high performance system laser treatment in men with benign prostatic hyperplasia. Korean J Urol 53:472–477. https://doi.org/10.4111/kju.2012.53.7.472
Kim KS, Choi SW, Bae WJ et al (2015) Efficacy of a vaporization–resection of the prostate median lobe enlargement and vaporization of the prostate lateral lobe for benign prostatic hyperplasia using a 120-W GreenLight high-performance system laser: the effect on storage symptoms. Lasers Med Sci 30:1387–1393. https://doi.org/10.1007/s10103-015-1740-7
Hojgaard M, Mikines KJ (2010) Ureteral injuries during photoselective vaporization of the prostate. Scand J UrolNephrol 44:265–268. https://doi.org/10.3109/00365591003645712
Gu X, Strom K, Spaliviero M, Wong C (2013) Does prostate configuration affect the efficacy and safety of GreenLightHPSTM laser photoselective vaporization prostatectomy (PVP)? Lasers Med Sci 28:473–478. https://doi.org/10.1007/s10103-012-1085-4
Kim MS, Park KK, Chung BH, Lee SH (2013) Effect of photoselective vaporization prostatectomy on lower urinary tract symptoms in benign prostatic hyperplasia with or without intravesical prostatic protrusion. Korean J Urol 54:36–41. https://doi.org/10.4111/kju.2013.54.1.36
Law K, Tholomier C, Couture F et al (2020) PD61-07 Global Greenlight Group. J Urol. https://doi.org/10.1097/ju.0000000000000978.07
Gratzke C, Bachmann A, Descazeaud A et al (2015) EAU guidelines on the assessment of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. EurUrol 67:1099–1109. https://doi.org/10.1016/j.eururo.2014.12.038
Nickel JC, Aaron L, Barkin J et al (2018) Canadian Urological Association guideline on male lower urinary tract symptoms/benign prostatic hyperplasia (MLUTS/BPH): 2018 update. Can UrolAssoc J 12:303–312. https://doi.org/10.5489/cuaj.5616
Eri LM, Thomassen H, Brennhovd B, Håheim LL (2002) Accuracy and repeatability of prostate volume measurements by transrectal ultrasound. Prostate Cancer Prostatic Dis 5:273–278. https://doi.org/10.1038/sj.pcan.4500568
Wang X (2014) Firth logistic regression for rare variant association tests. Front Genet 5:187. https://doi.org/10.3389/fgene.2014.00187
Doo CK, Uh HS (2009) Anatomic configuration of prostate obtained by noninvasive ultrasonography can predict clinical voiding parameters for determining BOO in men with LUTS. Urology 73:232–236. https://doi.org/10.1016/j.urology.2008.09.055
Zheng J, Pan J, Qin Y et al (2015) Role for intravesical prostatic protrusion in lower urinary tract symptom: a fluid structural interaction analysis study. BMC Urol 15:1–9. https://doi.org/10.1186/s12894-015-0081-y
Mariappan P, Brown DJG, McNeill AS (2007) Intravesical prostatic protrusion is better than prostate volume in predicting the outcome of trial without catheter in white men presenting with acute urinary retention: a prospective clinical study. J Urol 178:573–577. https://doi.org/10.1016/j.juro.2007.03.116
Park HY, Lee JY, Park SY et al (2012) Efficacy of alpha blocker treatment according to the degree of intravesical prostatic protrusion detected by transrectal ultrasonography in patients with benign prostatic hyperplasia. Korean J Urol 53:92–97. https://doi.org/10.4111/kju.2012.53.2.92
Yoshida T, Kinoshita H, Yoshida K et al (2016) Intravesical prostatic protrusion as a predicting factor for the adverse clinical outcome in patients with symptomatic benign prostatic enlargement treated with dutasteride. Urology 91:154–157. https://doi.org/10.1016/j.urology.2016.01.009
Funding
None.
Author information
Authors and Affiliations
Contributions
DDN protocol/project development, data collection or management, data analysis, manuscript writing/editing. IS protocol/project development, data collection or management, data analysis, manuscript writing/editing. KL protocol/project development, data collection or management, manuscript writing/editing. NB protocol/project development, manuscript writing/editing. DSE: Protocol/project development, manuscript writing/editing. ASZ protocol/project development, manuscript writing/editing. AA protocol/project development, manuscript writing/editing. FB Protocol/project development, manuscript writing/editing. LC protocol/project development, manuscript writing/editing. GF protocol/project development, manuscript writing/editing. CVL protocol/project development, manuscript writing/editing. TBB protocol/project development, manuscript writing/editing. EFB protocol/project development, manuscript writing/editing. HC protocol/project development, manuscript writing/editing. MR protocol/project development, manuscript writing/editing. ER protocol/project development, manuscript writing/editing. VM protocol/project development, manuscript writing/editing. KCZ protocol/project development, data collection or management, data analysis, manuscript writing/editing.
Corresponding author
Ethics declarations
Conflict of interest
Consultants and proctors for Boston Scientific for greenlight: KZ, DSE, VM, ER, HC. Investigators and consultants for PROCEPT BioRobotics: VM, TB, NB, KZ. Surgical tutors for Greenlight Xcelerated Performance System (American Medical System-AMS, Minnetonka, MN) and received honoraria for their tutorship: GF, LC. All other authors do not report any relevant conflicts of interest.
Ethics approval
All procedures performed in this study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
For this type of study, formal consent is not required (retrospective study).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Nguyen, DD., Sadri, I., Law, K. et al. Impact of the presence of a median lobe on functional outcomes of greenlight photovaporization of the prostate (PVP): an analysis of the Global Greenlight Group (GGG) Database. World J Urol 39, 3881–3889 (2021). https://doi.org/10.1007/s00345-020-03529-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-020-03529-w