
Abstract
Objective
To investigate the sexual, physical, and mental adverse effects associated with exposure to 5-alpha reductase inhibitors (5ARIs).
Methods
FAERS data containing finasteride and dutasteride reports were analyzed from January 2000 to April 2019. Reports identified one or more adverse effects, along with all concurrent medications. Cases of monotherapy of finasteride or dutasteride were identified. We conducted a chi-square test of independence to assess the relationship between the three drug groups and adverse event (AE) occurrence across 19 sexual, physical, and mental AE categories. The frequency procedure in SAS was utilized to summarize rates of AEs between various dosages of each drug.
Results
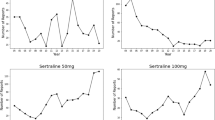
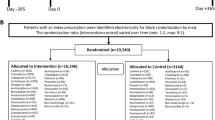
A total of 16,014 case reports were obtained. After excluding females, 7436 case reports of 5ARI monotherapy were identified: 2628 of dutasteride 0.5 mg, 3266 of finasteride 1 mg, and 744 of finasteride 5 mg. Differences in rates of AEs occurrence were statistically significant across all 19 variables (p < 0.001) with a significantly higher proportion of AEs attributed to finasteride 1 mg, with gynecomastia being the only exception. Case report submissions rose dramatically following FDA-mandated finasteride label change.
Conclusions
Analysis of FAERS data suggests AEs of 5ARIs are dose-independent with greater likelihood of occurrence in younger patients, particularly in sexual and mental domains. The causality and the rate of AEs are not certain based on the FAERS data and future prospective studies are necessary to determine the true rates.





Similar content being viewed by others

Change history
01 September 2021
A Correction to this paper has been published: https://doi.org/10.1007/s00345-021-03824-0
References
Liu L, Zhao S, Li F et al (2016) Effect of 5α-reductase inhibitors on sexual function: a meta-analysis and systematic review of randomized controlled trials. J Sex Med 13:1297–1310
Total Patient Tracker (TPT) Years 2002-2009. SDI Vector One®. Data extracted May, 2011. https://www.accessdata.fda.gov/drugsatfda_docs/nda/2009/020592Orig1s040s041OtherR.pdf
U.S. Food and Drug Administration. FDA Drug Safety Communication: 5-alpha reductase inhibitors (5-ARIs) may increase the risk of a more serious form of prostate cancer [Internet]. U.S. Food and Drug Administration, Silver Spring, c2013. Version 03/2013. 10]. http://www.fda.gov/Drugs/DrugSafety/ucm258314.htm
Ganzer CA, Jacobs AR, Iqbal F (2015) Persistent sexual, emotional, and cognitive impairment post-finasteride: a survey of men reporting symptoms. Am J Mens Health 9:222–228
Traish AM (2020) Post-finasteride syndrome: a surmountable challenge for clinicians. Fertil Steril 113:21–50
NIH (2015) Adverse events of 5-α-reductase inhibitors: US Department of Health and Human Services. Version 03/03/2015. https://rarediseases.info.nih.gov/diseases/12407/adverse-events-of-5-alpha-reductase-inhibitors
Administration USFD (2018) Questions and answers on FDA’s adverse event reporting system (FAERS). Version 06/04/2018. https://www.fda.gov/drugs/surveillance/questions-and-answers-fdas-adverse-event-reporting-system-faers
Ali AK (2011) Pharmacovigilance analysis of adverse event reports for aliskiren hemifumarate, a first-in-class direct renin inhibitor. Ther Clin Risk Manag 7:337–344
Golan DETJA, Armstrong EJ, Armstrong AW (2011) Principles of pharmacology: the pathophysiologic basis of drug therapy, 3rd revised international ed edition ed. Lippincott Williams and Wilkins, Philadelphia
Ali AK, Heran BS, Etminan M (2015) Persistent sexual dysfunction and suicidal ideation in young men treated with low-dose finasteride: a pharmacovigilance study. Pharmacotherapy 35:687–695
Mondaini N, Gontero P, Giubilei G et al (2007) Finasteride 5 mg and sexual side effects: How many of these are related to a nocebo phenomenon? J Sex Med 4:1708–1712
Olsen EA, Hordinsky M, Whiting D et al (2006) The importance of dual 5α-reductase inhibition in the treatment of male pattern hair loss: results of a randomized placebo-controlled study of dutasteride vs. finasteride. J Am Acad Dermatol 55:1014–1023
Rittmaster RS, Lemay A, Zwicker H et al (1992) Effect of finasteride, a 5α-reductase inhibitor, on serum gonadotropins in normal men. J Clin Endocrinol Metab 75:484–488
Clark RV, Hermann DJ, Cunningham GR, Wilson TH, Morrill BB, Hobbs S (2004) Marked suppression of dihydrotestosterone in men with benign prostatic hyperplasia by dutasteride, a dual 5α-reductase inhibitor. J Clin Endocrinol Metab 89:2179–2184
Wessells H, Roy J, Bannow J et al (2003) Incidence and severity of sexual adverse experiences in finasteride and placebo-treated men with benign prostatic hyperplasia. Urology 61:579–584
Physicians AAFP (2012) Finasteride sexual side effects prompt FDA warning, Label Changes. Version 04/18/2012. https://www.aafp.org/news/health-ofthe-public/20120418finasteride.html
Traish AM, Hassani J, Guay AT, Zitzmann M, Hansen ML (2011) Adverse side effects of 5α-reductase inhibitors therapy: persistent diminished libido and erectile dysfunction and depression in a subset of patients. J Sex Med 8:872–884
Mulhall JP, Luo X, Zou KH, Stecher V, Galaznik A (2016) Relationship between age and erectile dysfunction diagnosis or treatment using real-world observational data in the USA. Int J Clin Pract 70:1012–1018
Johannes CB, Araujo AB, Feldman HA, Derby CA, Kleinman KP, McKinlay JB (2000) Incidence of erectile dysfunction in men 40 to 69 years old: longitudinal results from the Massachusetts male aging study. J Urol 163:460–463
Moreira ED Jr, Lbo CF, Diament A, Nicolosi A, Glasser DB (2003) Incidence of erectile dysfunction in men 40 to 69 years old: results from a population-based cohort study in Brazil. Urology 61:431–436
Lim KB (2017) Epidemiology of clinical benign prostatic hyperplasia. Asian J Urol 4:148–151
Eisenberg ML, Meldrum D (2017) Effects of age on fertility and sexual function. Fertil Steril 107:301–304
Erectile dysfunction epidemiology (2003) Int J Impot Res 15(Suppl 7):S2–4
Morin L, Johnell K, Laroche ML, Fastbom J, Wastesson JW (2018) The epidemiology of polypharmacy in older adults: register-based prospective cohort study. Clin Epidemiol 10:289–298
Fourcade R, Lacoin F, Slama A, Gaudin A, Le Fur C, Michel E, Sitbon, Cotté (2010) UP-1.09: impact of benign prostatic hyperplasia (BPH) on medically treated patients' quality of life. Urology 76(3):S55
Cash TF (1999) The psychosocial consequences of androgenetic alopecia: a review of the research literature. Br J Dermatol 141:398–405
Wells PA, Willmoth T, Russell RJ (1995) Does fortune favour the bald? Psychological correlates of hair loss in males. Br J Psychol 86(Pt 3):337–344
Baas WR, Butcher MJ, Lwin A et al (2018) A review of the FAERS data on 5-α reductase inhibitors: implications for postfinasteride syndrome. Urology 120:143–149
Author information
Authors and Affiliations
Contributions
MBH: data collection/management/analysis, and manuscript writing. KH: data collection/management/analysis, and manuscript writing. AET: manuscript editing. SAK: manuscript editing. BC: protocol/project development, and manuscript writing/editing.
Corresponding author
Ethics declarations
Conflict of interest
The author(s) declare that they have no conflict of interest.
Research involving human participants
The data used in this study are de-identified and publicly available FAERS data. It has been determined by the Institutional Review Board (IRB) at Weill Cornell Medical College that it meets eligibility for IRB review exemption authorized by 45 CFR part 46.
Informed consent
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Harrell, M.B., Ho, K., Te, A.E. et al. An evaluation of the federal adverse events reporting system data on adverse effects of 5-alpha reductase inhibitors. World J Urol 39, 1233–1239 (2021). https://doi.org/10.1007/s00345-020-03314-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-020-03314-9