
Abstract
Purpose
This study aimed at evaluating whether removal of the ureteral stent the day before scheduled secondary intervention facilitates spontaneous ureteral stone passage and thus can spare the pre-stented patient this surgery.
Methods
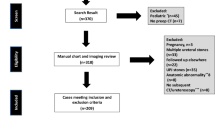
Retrospective analysis of a single-centre consecutive series of 216 patients after previous stenting due to a symptomatic ureteral stone from 01/2013 to 01/2018. Indwelling stents were removed under local anaesthesia. Patients were told to filter their urine overnight. Multivariate analysis was performed to assess predictive factors for spontaneous stone passage.
Results
34% (74/216) of patients had spontaneous stone passage while the stent was indwelling. Of the remaining 142 patients, 41% (58/142) had spontaneous stone passage within 24 h after stent removal. Only 84/216 (39%) patients needed secondary intervention. Multivariate logistic regression analysis of all 216 patients showed a significant association between spontaneous stone passage and smaller stone size (p < 0.001), distal stone location (p = 0.046) and stent dwell time (p = 0.02). Predictive factors for spontaneous stone passage after stent removal were smaller size (p < 0.001), distal location (p = 0.001), and stone movement while the stent was indwelling (p = 0.016). A treatment strategy was established that helps select patients suitable for conservative management.
Conclusions
The majority (61%) of ureteral stones passed spontaneously after pre-stenting; 34% while the stent was indwelling, 27% within 24 h after stent removal. Besides distal stone location, stone size (< 6 mm) and stone movement (≥ 5 cm) while the stent is indwelling indicate patients who are likely to pass their ureteral stone spontaneously after stent removal. The treatment strategy (decision tree) presented here helps identify those patients.
Trial registration

Similar content being viewed by others

References
Scales CD Jr, Smith AC, Hanley JM, Saigal CS (2012) Urologic diseases in America project. Prevalence of kidney stones in the United States. Eur Urol 62:160–165
Parks JH, Coe FL (1994) An increasing number of calcium oxalate stone events worsens treatment outcome. Kidney Int 45:1722–1730
Skolarikos A, Laguna MP, Alivizatos G, Kural AR, de la Rosette JJ (2010) The role for active monitoring in urinary stones: a systematic review. J Endourol 24:923–930
Bader MJ, Eisner B, Porpiglia F, Preminger GM, Tiselius H-G (2012) Contemporary management of ureteral stones. Eur Urol 61:764–772
European Association of Urology (EAU) Guidelines on Urolithiasis: https://uroweb.org/guideline/urolithiasis/
Assimos D, Crisci A, Culkin D et al (2016) Preoperative JJ stent placement in ureteric and renal stone treatment: results from the Clinical Research Office of Endourological Society (CROES) ureteroscopy (URS) Global Study. BJU Int 117:648–654
Jessen JP, Breda A, Brehmer M et al (2016) International collaboration in endourology: multicenter evaluation of prestenting for ureterorenoscopy. J Endourol 30:268–273
Jones BJ, Ryan PC, Lyons O, Grainger R, McDermott TE, Butler MR (1990) Use of the double pigtail stent in stone retrieval following unsuccessful ureteroscopy. Br J Urol 66:254–256
Lennon GM, Thornhill JA, Grainger R, McDermott TE, Butler MR (1997) Double pigtail ureteric stent versus percutaneous nephrostomy: effects on stone transit and ureteric motility. Eur Urol 31:24–29
Baumgarten L, Desai A, Shipman S et al (2017) Spontaneous passage of ureteral stones in patients with indwelling ureteral stents. Can J Urol 24:9024–9029
Millman S, Strauss AL, Parks JH, Coe FL (1982) Pathogenesis and clinical course of mixed calcium oxalate and uric acid nephrolithiasis. Kidney Int 22:366–370
Nakada SY, Hoff DG, Attai S, Heisey D, Blankenbaker D, Pozniak M (2000) Determination of stone composition by noncontrast spiral computed tomography in the clinical setting. Urology 55:816–819
Becker G (2007) Uric acid stones. Nephrology 12:S21–25
Venkatesh R, Landman J, Minor SD et al (2005) Impact of a double-pigtail stent on ureteral peristalsis in the porcine model: initial studies using a novel implantable magnetic sensor. J Endourol 19:170–176
Ryan PC, Lennon GM, McLean PA, Fitzpatrick JM (1994) The effects of acute and chronic JJ stent placement on upper urinary tract motility and calculus transit. Br J Urol 74:434–439
Taha DE, Elshal AM, Zahran MH, Harraz AM, El-Nahas AR, Shokeir AA (2015) After urgent drainage of an obstructed kidney by internal ureteric stenting: is ureteroscopic stone extraction always needed? Arab J Urol 13:258–263
Türk C, Knoll T, Seitz C, Skolarikos A, Chapple C, McClinton S (2017) European Association of Urology. Medical expulsive therapy for ureterolithiasis: the EAU recommendations in 2016. Eur Urol 71:504–507
Loftus C, Nyame Y, Hinck B et al (2016) Medical expulsive therapy is underused for the management of renal colic in the emergency setting. J Urol 195:987–991
Davenport K, Timoney AG, Keeley FX (2006) A comparative in vitro study to determine the beneficial effect of calcium-channel and alpha(1)-adrenoceptor antagonism on human ureteric activity. BJU Int 98:651–655
Moradi M, Abdi H, Ebrahimi S, Rezaee H, Kaseb K (2017) Effects of Tamsulosin and Tolterodine on double J stent-related symptoms: a double-blind, randomized, placebo-controlled trial. SAGE Open Med 5:2050312117696436
Pais VM Jr, Smith RE, Stedina EA, Rissman CM (2016) Does omission of ureteral stents increase risk of unplanned return visit? A systematic review and meta-analysis. J Urol 196:1458–1466
Joshi HB, Stainthorpe A, MacDonagh RP, Keeley FX Jr, Timoney AG, Barry MJ (2003) Indwelling ureteral stents: evaluation of symptoms, quality of life and utility. J Urol 169:1065–1069
Lee C, Kuskowski M, Premoli J, Skemp N, Monga M (2005) Randomized evaluation of ureteral stents using validated symptom questionnaire. J Endourol 19:990–993
Funding
There was no direct or indirect commercial incentive associated with publishing the article.
Author information
Authors and Affiliations
Contributions
ESG: data collection, manuscript writing, data analysis. TG: data collection, manuscript editing. MAF: data management, manuscript editing. PB: data analysis, manuscript editing. BK: manuscript editing. MDV: data analysis, manuscript editing. BR: project and protocol development, data management and collection, data analysis, manuscript writing and editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Statement of human rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was conducted in accordance with the “Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE) statement and approved by the Ethics Committee of the Canton Bern, Switzerland (protocol number: KEK-Be 2017-01698).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Stojkova Gafner, E., Grüter, T., Furrer, M.A. et al. A treatment strategy to help select patients who may not need secondary intervention to remove symptomatic ureteral stones after previous stenting. World J Urol 38, 2955–2961 (2020). https://doi.org/10.1007/s00345-020-03087-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-020-03087-1