
Abstract
Purpose
To compare perioperative outcomes and complications of extracorporeal (ECUD) vs intracorporeal urinary diversion (ICUD) in patients after undergoing robot-assisted radical cystectomy (RARC) at five referral centers in France.
Methods
We retrospectively reviewed our multi-institutional, prospectively-collected database to select patients undergoing RARC between 2010 and 2016 with at least 3 months of follow-up. At each center, the surgery was performed by one surgeon with extensive experience in robotic surgery and radical cystectomy but no prior experience in RARC.
Results
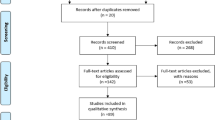
Overall, 108 patients were included. ECUD and ICUD were performed in 34 (31.5%) and 74 (68.5%) patients, respectively. Patient characteristics were comparable among the two groups, except for a higher proportion of patients with high surgical risk (ASA score ≥ 3) in the ECUD group. Ileal conduit and ileal neobladder were performed in 63/108 (58%) and 45/108 (42%) cases, respectively. Ileal conduit was performed more often with an extracorporeal approach while ileal neobladder with an intracorporeal approach. Overall, operative time, length of hospital stay, positive margin rate, and number of lymph nodes removed did not significantly differ among the two cohorts. Estimated blood loss and transfusion rates were significantly higher in the ECUD group. Rate of early (38.2 vs 47.3%, p = 0.4) and late (29.4 vs 18.9%, p = 0.2) surgical complications did not significantly differ between the ECUD and ICUD groups. Results were comparable in the subgroup analysis in the ileal conduit subpopulation.
Conclusion
In our real-life, multi-institutional study, RARC with ICUD achieved perioperative outcomes and complication rates comparable to those of RARC with ECUD.
Similar content being viewed by others

References
Witjes AJ, Lebret T, Compérat EM et al (2017) Updated 2016 EAU guidelines on muscle-invasive and metastatic bladder cancer. Eur Urol 71:462–475
Chang SS, Bochner BH, Chou R et al (2017) Treatment of non-metastatic muscle-invasive bladder cancer: Aua/Asco/Astro/Suo guideline. J Urol 198:552–559
Milowsky MI, Rumble RB, Booth CM et al (2016) Guideline on muscle-invasive and metastatic bladder cancer (European Association of Urology Guideline): American Society of Clinical Oncology Clinical Practice Guideline Endorsement. J Clin Oncol 34:1945–1952
Hu JC, Chughtai B, O’Malley P et al (2016) Perioperative outcomes, health care costs, and survival after robotic-assisted versus open radical cystectomy: a national comparative effectiveness study. Eur Urol 70:195–202
Hussein AA, May PR, Jing Z et al (2018) Outcomes of intracorporeal urinary diversion after robot-assisted radical cystectomy: results from the International Robotic Cystectomy Consortium. J Urol. https://doi.org/10.1016/j.juro.2017.12.045 (in press)
Leow JJ, Reese SW, Jiang W et al (2014) Propensity-matched comparison of morbidity and costs of open and robot-assisted radical cystectomies: a contemporary population-based analysis in the United States. Eur Urol 66:569–576
Novara G, Catto JW, Wilson T et al (2015) Systematic review and cumulative analysis of perioperative outcomes and complications after robot-assisted radical cystectomy. Eur Urol 67:376–401
Yuh B, Wilson T, Bochner B et al (2015) Systematic review and cumulative analysis of oncologic and functional outcomes after robot-assisted radical cystectomy. Eur Urol 67:402–422
Wilson TG, Guru K, Rosen RC et al (2015) Best practices in robot-assisted radical cystectomy and urinary reconstruction: recommendations of the Pasadena Consensus Panel. Eur Urol 67:363–375
Ahmed K, Khan SA, Hayn MH et al (2014) Analysis of intracorporeal compared with extracorporeal urinary diversion after robot-assisted radical cystectomy: results from the International Robotic Cystectomy Consortium. Eur Urol 65:340–347
Roghmann F, Becker A, Trinh QD et al (2013) Updated assessment of neobladder utilization and morbidity according to urinary diversion after radical cystectomy: a contemporary US-population-based cohort. Can Urol Assoc J 7:E552–E560
Azzouni FS, Din R, Rehman S et al (2013) The first 100 consecutive, robot-assisted, intracorporeal ileal conduits: evolution of technique and 90-day outcomes. Eur Urol 63:637–643
Collins JW, Tyritzis S, Nyberg T et al (2014) Robot-assisted radical cystectomy (Rarc) with intracorporeal neobladder—what is the effect of the learning curve on outcomes? BJU Int 113:100–107
Kang SG, Ko YH, Jang HA et al (2012) Initial experience of robot-assisted radical cystectomy with total intracorporeal urinary diversion: comparison with extracorporeal method. J Laparoendosc Adv Surg Tech A 22:456–463
Mitropoulos D, Artibani W, Graefen M et al (2012) Reporting and grading of complications after urologic surgical procedures: an ad hoc EAU guidelines panel assessment and recommendations. Eur Urol 61:341–349
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Humphrey PA, Moch H, Cubilla AL et al (2016) The 2016 WHO classification of tumours of the urinary system and male genital organs—part B: prostate and bladder tumours. Eur Urol 70:106–119
Gierth M, Aziz A, Fritsche HM et al (2014) The effect of intra- and postoperative allogenic blood transfusion on patients’ survival undergoing radical cystectomy for urothelial carcinoma of the bladder. World J Urol 32:1447–1453
Linder BJ, Frank I, Cheville JC et al (2013) The impact of perioperative blood transfusion on cancer recurrence and survival following radical cystectomy. Eur Urol 63:839–845
Gore JL, Yu HY, Setodji C et al (2010) Urinary diversion and morbidity after radical cystectomy for bladder cancer. Cancer 116:331–339
Jahnson S, Damm O, Hellsten S et al (2010) Urinary diversion after cystectomy for bladder cancer: a population based study in Sweden. Scand J Urol Nephrol 44:69–75
Bader P, Westermann D, Frohneberg D (2009) Urinary diversions: which one is right for which patient? Urologe A 48:127–136
Mottet N, Castagnola C, Rischmann P et al (2008) Quality of life after cystectomy: French national survey conducted by the French Association of Urology (AFU), the French Federation of Stoma Patients (FSF) and the French Association of Enterostomy Patients (AFET) in patients with ileal conduit urinary diversion or orthotopic neobladder. Prog Urol 18:292–298
Colombo R, Naspro R (2010) Ileal conduit as the standard for urinary diversion after radical cystectomy for bladder cancer. Eur Urol Suppl 9:736–744
Author information
Authors and Affiliations
Contributions
LL: data collection and manuscript writing. GV: data collection. RC: manuscript writing. JP: manuscript editing. VG: data collection. AM-L: data collection. DV: data collection. AT: manuscript editing. MR: data collection. ML: data collection. LT: manuscript editing. VM: manuscript editing. PG: manuscript editing. CV: manuscript editing. GP: manuscript editing. BG: data analysis. MR: project development and manuscript editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Research involving human participants
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and national research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
345_2018_2313_MOESM1_ESM.docx
Supplementary Table 1. Clinical characteristics, perioperative outcomes and complication rates of patients excluded from the study due to intraoperative conversion from robot-assisted radical cystectomy (RARC) to open radical cystectomy (n=9) (DOCX 16 kb)
Rights and permissions
About this article

Cite this article
Lenfant, L., Verhoest, G., Campi, R. et al. Perioperative outcomes and complications of intracorporeal vs extracorporeal urinary diversion after robot-assisted radical cystectomy for bladder cancer: a real-life, multi-institutional french study. World J Urol 36, 1711–1718 (2018). https://doi.org/10.1007/s00345-018-2313-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-018-2313-8