
Abstract
Purpose
To identify computed tomography (CT) findings associated with successful conservative treatment of closed loop small bowel obstruction (CL-SBO) due to adhesions or internal herniation.
Material and methods
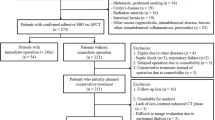
The local institutional review board approved this study while waiving informed consent. Clinical and CT data were collected retrospectively for 96 consecutive patients with a CT diagnosis of CL-SBO due to adhesions or internal herniation established by experienced radiologists who had no role in patient management. Mechanical obstruction with at least two transition zones on the bowel at a single site defined CL-SBO. Two radiologists blinded to patient data independently performed a retrospective review of the CT scans. The patient groups with successful versus failed initial conservative therapy were compared. Univariate and multivariate analyses were performed to look for CT findings associated with successful conservative therapy. Interobserver agreement was assessed for each CT finding.
Results
Of the 96 patients, 34 (35%) underwent immediate surgery and 62 (65%) received first-line conservative treatment, which succeeded in 19 (31%) and failed in 43 (69%). The distance between the transition zones was the only independent predictor of successful conservative therapy (odds ratio, 4.6 when ≥ 8 mm; 95% confidence interval [95% CI], 1.2–18.3). A distance ≥ 8 mm had 84% (95% CI, 60–97) sensitivity and 46% (95% CI, 31–62) specificity for successful conservative treatment. The correlation coefficient for the distance between transition zones between readers 1 and 2 was fair (r = 0.46).
Conclusion
CL-SBO can be resolved without surgery. When there is no CT sign of ischemia, the distance between the transition zones should be assessed.
Key Points
• Twenty percent (19/96) of all cases of closed loop small bowel obstruction (CL-SBO) representing 31% of the patients given first-line conservative therapy, were resolved without surgery.
• The distance between the transition zones may help to choose between conservative and surgical management in patients with a CL-SBO but no CT evidence of ischemia.
• A distance < 8 mm between the transition zones suggests a need for emergent surgery.




Similar content being viewed by others


Abbreviations
- CL-SBO:
-
Closed loop small bowel obstruction
- CT:
-
Computed tomography
- SBO:
-
Small bowel obstruction
References
Balthazar EJ, Birnbaum BA, Megibow AJ, Gordon RB, Whelan CA, Hulnick DH (1992) Closed-loop and strangulating intestinal obstruction: CT signs. Radiology. 185(3):769–775
Balthazar EJ, Liebeskind ME, Macari M (1997) Intestinal ischemia in patients in whom small bowel obstruction is suspected: evaluation of accuracy, limitations, and clinical implications of CT in diagnosis. Radiology. 205(2):519–522
Millet I, Boutot D, Faget C et al (2017) Assessment of strangulation in adhesive small bowel obstruction on the basis of combined CT findings: implications for clinical care. Radiology 285(3):798–808
Elsayes KM, Menias CO, Smullen TL, Platt JF (2007) Closed-loop small-bowel obstruction: diagnostic patterns by multidetector computed tomography. J Comput Assist Tomogr 31(5):697–701
Makar RA, Bashir MR, Haystead CM et al (2016) Diagnostic performance of MDCT in identifying closed loop small bowel obstruction. Abdom Radiol (NY) 41(7):1253–1260
Zielinski MD, Eiken PW, Bannon MP et al (2010) Small bowel obstruction-who needs an operation? A multivariate prediction model. World J Surg 34(5):910–919
Chang WC, Ko KH, Lin CS et al (2014) Features on MDCT that predict surgery in patients with adhesive-related small bowel obstruction. PLoS One 9(2):e89804
Makita O, Ikushima I, Matsumoto N, Arikawa K, Yamashita Y, Takahashi M (1999) CT differentiation between necrotic and nonnecrotic small bowel in closed loop and strangulating obstruction. Abdom Imaging 24(2):120–124
Kato K, Mizunuma K, Sugiyama M et al (2010) Interobserver agreement on the diagnosis of bowel ischemia: assessment using dynamic computed tomography of small bowel obstruction. Jpn J Radiol 28(10):727–732
Maglinte DD, Gage SN, Harmon BH et al (1993) Obstruction of the small intestine: accuracy and role of CT in diagnosis. Radiology. 188(1):61–64
Nakashima K, Ishimaru H, Fujimoto T et al (2015) Diagnostic performance of CT findings for bowel ischemia and necrosis in closed-loop small-bowel obstruction. Abdom Imaging 40(5):1097–1103
Ten Broek RPG, Krielen P, Di Saverio S et al (2018) Bologna guidelines for diagnosis and management of adhesive small bowel obstruction (ASBO): 2017 update of the evidence-based guidelines from the world society of emergency surgery ASBO working group. World J Emerg Surg 13:24
Rondenet C, Millet I, Corno L, Boulay-Coletta I, Taourel P, Zins M (2018) Increased unenhanced bowel-wall attenuation: a specific sign of bowel necrosis in closed-loop small-bowel obstruction. Eur Radiol 28(10):4225–4233
Millet I, Taourel P, Ruyer A, Molinari N (2015) Value of CT findings to predict surgical ischemia in small bowel obstruction: a systematic review and meta-analysis. Eur Radiol 25(6):1823–1835
Geffroy Y, Boulay-Coletta I, Jullès MC, Nakache S, Taourel P, Zins M (2014) Increased unenhanced bowel-wall attenuation at multidetector CT is highly specific of ischemia complicating small-bowel obstruction. Radiology. 270(1):159–167
Sheedy SP, Earnest F 4th, Fletcher JG, Fidler JL, Hoskin TL (2006) CT of small-bowel ischemia associated with obstruction in emergency department patients: diagnostic performance evaluation. Radiology. 241(3):729–736
Khaled W, Millet I, Corno L et al (2018) Clinical relevance of the feces sign in small-bowel obstruction due to adhesions depends on its location. AJR Am J Roentgenol 210(1):78–84
Millet I, Ruyer A, Alili C et al (2014) Adhesive small-bowel obstruction: value of CT in identifying findings associated with the effectiveness of nonsurgical treatment. Radiology. 273(2):425–432
Cohen JF, Korevaar DA, Altman DG et al (2016) STARD 2015 guidelines for reporting diagnostic accuracy studies: explanation and elaboration. BMJ Open 6(11):e012799
Balthazar EJ (1994) George W. Holmes Lecture. CT of small-bowel obstruction. AJR Am J Roentgenol 162(2):255–261
Chou CK (2002) CT manifestations of bowel ischemia. AJR Am J Roentgenol 178(1):87–91
Yen CH, Chen JD, Tui CM et al (2005) Internal hernia: computed tomography diagnosis and differentiation from adhesive small bowel obstruction. J Chin Med Assoc 68(1):21–28
Funding
The authors state that this work has not received any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Dr. Marc Zins.
Conflict of interest
The authors declare that they have no conflict of interest.
Statistics and biometry
One of the authors has significant statistical expertise.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Ethical approval
Institutional Review Board approval was obtained.
Study subjects or cohorts overlap
Some study subjects (43%) have been previously reported in a published article: C. Rondenet, Eur Radiol, 2018.
Methodology
• retrospective
• diagnostic study
• performed at one institution
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Rondenet, C., Millet, I., Corno, L. et al. CT diagnosis of closed loop bowel obstruction mechanism is not sufficient to indicate emergent surgery. Eur Radiol 30, 1105–1112 (2020). https://doi.org/10.1007/s00330-019-06413-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-019-06413-3