
Abstract
Objectives
To analyse the implementation, applicability and accuracy of the pretest probability calculation provided by NICE clinical guideline 95 for decision making about imaging in patients with chest pain of recent onset.
Methods
The definitions for pretest probability calculation in the original Duke clinical score and the NICE guideline were compared. We also calculated the agreement and disagreement in pretest probability and the resulting imaging and management groups based on individual patient data from the Collaborative Meta-Analysis of Cardiac CT (CoMe-CCT).
Results
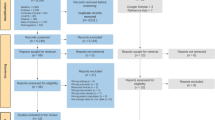
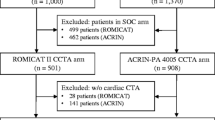
4,673 individual patient data from the CoMe-CCT Consortium were analysed. Major differences in definitions in the Duke clinical score and NICE guideline were found for the predictors age and number of risk factors. Pretest probability calculation using guideline criteria was only possible for 30.8 % (1,439/4,673) of patients despite availability of all required data due to ambiguity in guideline definitions for risk factors and age groups. Agreement regarding patient management groups was found in only 70 % (366/523) of patients in whom pretest probability calculation was possible according to both models.
Conclusions
Our results suggest that pretest probability calculation for clinical decision making about cardiac imaging as implemented in the NICE clinical guideline for patients has relevant limitations.
Key Points
• Duke clinical score is not implemented correctly in NICE guideline 95.
• Pretest probability assessment in NICE guideline 95 is impossible for most patients.
• Improved clinical decision making requires accurate pretest probability calculation.
• These refinements are essential for appropriate use of cardiac CT.

Similar content being viewed by others

Change history
01 June 2018
The original version of this article, published on 19 March 2018, unfortunately contained a mistake. The following correction has therefore been made in the original: The names of the authors Philipp A. Kaufmann, Ronny Ralf Buechel and Bernhard A. Herzog were presented incorrectly.
Abbreviations
- CACS:
-
Coronary artery calcium score
- CAD:
-
Coronary artery disease
- CoMe-CCT:
-
Collaborative Meta-Analysis of Cardiac CT
- CT:
-
Computed tomography
- CTA:
-
Computed tomography angiography
- ECG:
-
Exercise electrocardiogram
- ICA:
-
Invasive coronary angiography
- NICE:
-
National Institute for Health and Care Excellence
- PMG:
-
Patient management group
References
Fihn SD, Gardin JM, Abrams J et al (2012) ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation 126(25):e354–e471
Nichols M, Townsend N, Luengo-Fernandez R et al (2012) European Cardiovascular Disease Statistics 2012. Brussels European Heart Network, Brussels, European Society of Cardiology, Sophia Antipolis
Go AS, Mozaffarian D, Roger VL et al (2013) Heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation 127(1):e6–e245
Moschovitis A, Cook S, Meier B (2010) Percutaneous coronary interventions in Europe in 2006. EuroIntervention 6(2):189–194
Patel MR, Dai D, Hernandez AF et al (2014) Prevalence and predictors of nonobstructive coronary artery disease identified with coronary angiography in contemporary clinical practice. Am Heart J 167(6):846–52.e2
Montalescot G, Sechtem U, Achenbach S et al (2013) ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J 34(38):2949–3003
Leber AW, Johnson T, Becker A et al (2007) Diagnostic accuracy of dual-source multi-slice CT-coronary angiography in patients with an intermediate pretest likelihood for coronary artery disease. Eur Heart J 28(19):2354–2360
Schuetz GM, Zacharopoulou NM, Schlattmann P, Dewey M (2010) Meta-analysis: noninvasive coronary angiography using computed tomography versus magnetic resonance imaging. Ann Intern Med 152(3):167–177
Meijboom WB,Meijs MF, Schuijf JD et al (2008) Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol 52(25):2135–2144
von Ballmoos MW, Haring B, Juillerat P, Alkadhi H (2011) Meta-analysis: diagnostic performance of low-radiation-dose coronary computed tomography angiography. Ann Intern Med 154(6):413–420
Schlattmann P, Schuetz GM, Dewey M (2011) Influence of coronary artery disease prevalence on predictive values of coronary CT angiography: a meta-regression analysis. Eur Radiol 21(9):1904–1913
Cooper A, Calvert N, Skinner J et al (2010) Chest pain of recent onset: assessment and diagnosis of recent onset chest pain or discomfort of suspected cardiac origin. London: National Clinical Guideline Centre for Acute and Chronic Conditions
Pryor DB, Shaw L, McCants CB et al (1993) Value of the history and physical in identifying patients at increased risk for coronary artery disease. Ann Intern Med 118(2):81–90
Schuetz GM, Schlattmann P, Achenbach S et al (2013) Individual patient data meta-analysis for the clinical assessment of coronary computed tomography angiography: protocol of the Collaborative Meta-Analysis of Cardiac CT (CoMe-CCT). Syst Rev 2:13
Pryor DB, Harrell FE Jr, Lee KL, Califf RM, Rosati RA (1983) Estimating the likelihood of significant coronary artery disease. Am J Med 75(5):771–780
Diamond GA, Forrester JS (1979) Analysis of probability as an aid in the clinical diagnosis of coronary-artery disease. N Engl J Med 300(24):1350–1358
Genders TS, Steyerberg EW, Hunink MG et al (2012) Prediction model to estimate presence of coronary artery disease: retrospective pooled analysis of existing cohorts. BMJ 344:e3485
Cheng VY, Berman DS, Rozanski A et al (2011) Performance of the traditional age, sex, and angina typicality-based approach for estimating pretest probability of angiographically significant coronary artery disease in patients undergoing coronary computed tomographic angiography: results from the multinational coronary CT angiography evaluation for clinical outcomes: an international multicenter registry (CONFIRM). Circulation 124(22):2423–2432 1-8
Michail M, Lee AJX, Quaderi SA, Richardson JA, Aggarwal SK, Speechly-Dick ME (2013) Implementation of NICE Clinical Guideline 95 for investigation of "chest pain of recent onset" reduces cost. Eur Heart J 34:625
Kelly D, Cole S, Rossiter F, Mallinson K, Smith A, Simpson I (2011) Implementation of the new NICE guidelines for stable chest pain: likely impact on chest pain services in the UK. Br J Cardiol 18(4):185–188
Patterson C, Nicol E, Bryan L et al (2011) The effect of applying NICE guidelines for the investigation of stable chest pain on out-patient cardiac services in the UK. QJM 104(7):581–588
Rogers T, Dowd R, Yap HL, Claridge S, Al Fakih K, Byrne J (2013) Strict application of NICE Clinical Guideline 95 ‘chest pain of recent onset’ leads to over 90% increase in cost of investigation. Int J Cardiol 166(3):740–742
Patterson CM,Nair A, Ahmed N, Bryan L, Bell D, Nicol ED (2015) Clinical outcomes when applying NICE guidance for the investigation of recent-onset chest pain to a rapid-access chest pain clinic population. Heart 101(2):113–118
McKavanagh P, Lusk L, Ball PA, Trinick TR, Duly E, Walls GM (2013) A comparison of Diamond Forrester and coronary calcium scores as gatekeepers for investigations of stable chest pain. Int J Card Imaging 29(7):1547–1555
Pavitt CW, Harron K, Lindsay AC et al (2014) 147 Deriving Coronary Artery Calcium Scores from CT Coronary Angiography: A Potential for Change to the UK Nice Guidelines on Stable Chest Pain. Heart 100(Suppl 3):A85–A86
Genders TS, Steyerberg EW, Alkadhi H et al (2011) A clinical prediction rule for the diagnosis of coronary artery disease: validation, updating, and extension. Eur Heart J 32(11):1316–1330
Gunderman RB (2013) The story behind the image. Radiology 268(2):312–314
Krumholz HM (2013) Target cardiovascular risk rather than cholesterol concentration. BMJ 347:f7110
Zylka-Menhorn V (2013) Kurswechel löst heftigen Streit aus. Deutsches Ärzteblatt 110(50):A2425–A2426
Goff DC Jr, Lloyd-Jones DM, Bennett G et al (2014) 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 129(suppl 2):S49–S73
Funding
The authors of this manuscript state that the CoMe-CCT project received funding from the joint program of the German Research Foundation (DFG) and the German Federal Ministry of Education and Research (BMBF) for meta-analyses.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Marc Dewey.
Conflict of interest
All authors have completed the Unified Competing Interest form at www.icmje.org/disclosure.pdf (available on request from the corresponding author) and declare: RR, VW, PG, WBM, MG, HA, LH, NB, EZ, SL, BG, CR, AAS, BN, AS, MFLM, HB, SMMJ, KAØ, ACPD, AH, BAH, VMR, YLW, JR, MS, CL, SG, EM, HN, AS, KN, GU, ZZ, HM, MC, DAH, DB, RJ, KS, LY, TJ, JPL, RM, SM, JCT, DM, AdR and ML have nothing to disclose. GMS reports grants from German Federal Ministry of Education and Research (BMBF), during the conduct of the study. DA reports other from GE Healthcare, during the conduct of the study; other from GE Healthcare, outside the submitted work. GP reports other from General Electric, other from Bayer, other from Medtronic, other from Heartflow, outside the submitted work. JH reports grants from Siemens Medical Solutions, outside the submitted work. UJS reports grants from Bayer, grants from Bracco, grants from GE, grants from Medrad, grants from Siemens Healthcare, outside the submitted work. JK reports personal fees from Lantheus Inc, grants from Orion Pharma, outside the submitted work. KN reports non-financial support from Siemens Medical Solutions, grants from GE Healthcare, other from Toshiba Medical Systems, non-financial support from Abbott Vascular, grants from Bayer healthcare, outside the submitted work. PK, RRB, and BH report that the University Hospital Zurich holds a research contract with GE Healthcare. JL reports personal fees from GE Healthcare, personal fees from Heartflow, outside the submitted work. BC reports research grants from GE healthcare and educational support from TeraRecon, outside the submitted work. NP reports grants from Toshiba Medical System, outside the submitted work. JH reports grants and personal fees from Toshiba Medical Systems, during the conduct of the study. RH reports grants from Toshiba, outside the submitted work. PS reports grants from Ministry of Education and Research (BMBF) for meta-analyses as part of the joint programme "clinical trials" of the BMBF and the German Science Foundation (DFG), during the conduct of the study; grants from German Science Foundation (DFG), grants from European Union, outside the submitted work. MD has received grant support from the Heisenberg Program of the DFG for a professorship (DE 1361/14-1), the FP7 Program of the European Commission for the randomized multicentre DISCHARGE trial (603266-2, HEALTH-2012.2.4.-2), the European Regional Development Fund (20072013 2/05, 20072013 2/48), the German Heart Foundation/German Foundation of Heart Research (F/23/08, F/27/10), the Joint Program from the German Research Foundation (DFG) and the German Federal Ministry of Education and Research (BMBF) for meta-analyses (01KG1013, 01KG1110, 01KG1110), GE Healthcare, Bracco, Guerbet, and Toshiba Medical Systems. MD has also received lecture fees from Toshiba Medical Systems, Guerbet, Cardiac MR Academy Berlin, and Bayer (Schering-Berlex). MD is a consultant to Guerbet and one of the principal investigators of multicentre studies (CORE-64 and 320) on coronary CT angiography sponsored by Toshiba Medical Systems. He is also the editor of Coronary CT Angiography and Cardiac CT, both published by Springer, and offers hands-on workshops on cardiovascular imaging (www.ct-kurs.de). MD is an associate editor of Radiology and European Radiology. Institutional master research agreements exist with Siemens Medical Solutions, Philips Medical Systems, and Toshiba Medical Systems. The terms of these arrangements are managed by the legal department of Charité – Universitätsmedizin Berlin.
Statistics and biometry
No complex statistical methods were necessary for this paper.
Informed consent
Written informed consent was not required for this study because of the retrospective study design (meta-analysis).
Ethical approval
Institutional Review Board approval was not required because of the retrospective study design (meta-analysis).
Methodology
• diagnostic study
• individual patient data meta-analysis
• multicentre study
Additional information
The original version of this article was revised: The names of the authors Philipp A. Kaufmann, Ronny Ralf Buechel and Bernhard A. Herzog were presented incorrectly.
Rights and permissions
About this article

Cite this article
Roehle, R., Wieske, V., Schuetz, G.M. et al. Applicability and accuracy of pretest probability calculations implemented in the NICE clinical guideline for decision making about imaging in patients with chest pain of recent onset. Eur Radiol 28, 4006–4017 (2018). https://doi.org/10.1007/s00330-018-5322-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-018-5322-5