
Abstract
Objectives
The correlation between ultra low dose computed tomography (ULDCT)-detected parenchymal lung changes and pulmonary function abnormalities is not well described. This study aimed to determine the relationship between ULDCT-detected interstitial lung disease (ILD) and measures of pulmonary function in an asbestos-exposed population.
Methods
Two thoracic radiologists independently categorised prone ULDCT scans from 143 participants for ILD appearances as absent (score 0), probable (1) or definite (2) without knowledge of asbestos exposure or lung function. Pulmonary function measures included spirometry and diffusing capacity to carbon monoxide (DLCO).
Results
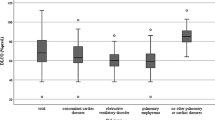
Participants were 92% male with a median age of 73.0 years. CT dose index volume was between 0.6 and 1.8 mGy. Probable or definite ILD was reported in 63 (44.1%) participants. Inter-observer agreement was good (k = 0.613, p < 0.001). There was a statistically significant correlation between the ILD score and both forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) (r = -0.17, p = 0.04 and r = -0.20, p = 0.02). There was a strong correlation between ILD score and DLCO (r = -0.34, p < 0.0001).
Conclusion
Changes consistent with ILD on ULDCT correlate well with corresponding reductions in gas transfer, similar to standard CT. In asbestos-exposed populations, ULDCT may be adequate to detect radiological changes consistent with asbestosis.
Key Points
• Interobserver agreement for the ILD score using prone ULDCT is good.
• Prone ULDCT appearances of ILD correlate with changes in spirometric observations.
• Prone ULDCT appearances of ILD correlate strongly with changes in gas transfer.
• Prone ULDCT may provide sufficient radiological evidence to inform the diagnosis of asbestosis.


Similar content being viewed by others

Abbreviations
- ARP:
-
Asbestos Review Program
- ATS:
-
American Thoracic Society
- CXR:
-
Chest x-ray
- DLCO:
-
Diffusion capacity of carbon monoxide
- ERS:
-
European Respiratory Society
- FEV1:
-
Forced expiratory volume in 1 s
- FVC:
-
Forced vital capacity
- HRCT:
-
High-resolution computed tomography
- ILD:
-
Interstitial lung disease
- IQR:
-
Interquartile range
- IPF:
-
Idiopathic pulmonary fibrosis
- LDCT:
-
Low-dose computed tomography
- SD:
-
Standard deviation
- UIP:
-
Usual interstitial pneumonitis
- ULDCT:
-
Ultra-low dose computed tomography
References
Staples CA, Gamsu G, Ray CS, Webb WR (1989) High resolution computed tomography and lung function in asbestos-exposed workers with normal chest radiographs. Am Rev Respir Dis 139:1502–1508
Remy-Jardin M, Sobaszek A, Duhamel A, Mastora I, Zanetti C, Remy J (2004) Asbestos-related pleuropulmonary diseases: evaluation with low-dose four–detector row spiral CT. Radiology 233:182–190
Lynch DA, Godwin JD, Safrin S et al (2005) High-resolution computed tomography in idiopathic pulmonary fibrosis: diagnosis and prognosis. Am J Respir Crit Care Med 172:488–493
Tashkin DP, Volkmann ER, Tseng CH et al (2014) Relationship between quantitative radiographic assessments of interstitial lung disease and physiological and clinical features of systemic sclerosis. Ann Rheum Dis. doi:10.1136/annrheumdis-2014-206076
Copley SJ, Lee YC, Hansell DM et al (2007) Asbestos-induced and smoking-related disease: apportioning pulmonary function deficit by using thin-section CT. Radiology 242:258–266
Roggli VL, Gibbs AR, Attanoos R et al (2010) Pathology of asbestosis- an update of the diagnostic criteria: report of the asbestosis committee of the college of American pathologists and pulmonary pathology society. Arch Pathol Lab Med 134:462–480
Aberle DR, Adams AM, Berg CD et al (2011) Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 365:395–409
Brims FJ, Murray CP, de Klerk N et al (2015) Ultra-low-dose chest computer tomography screening of an asbestos-exposed population in Western Australia. Am J Respir Crit Care Med 191:113–116
Murray CP, Wong PM, Teh J et al (2016) Ultra low dose CT screen-detected non-malignant incidental findings in the Western Australian Asbestos Review Programme. Respirology 21:1419–1424
Carrillo MC, Alturkistany S, Roberts H et al (2013) Low-dose computed tomography (LDCT) in workers previously exposed to asbestos: detection of parenchymal lung disease. J Comput Assist Tomogr 37:626–630
Hansen J, de Klerk NH, Eccles JL, Musk AW, Hobbs MS (1993) Malignant mesothelioma after environmental exposure to blue asbestos. Int J Cancer 54:578–581
Miller MR, Hankinson J, Brusasco V et al (2005) ATS/ERS Task Force: standardisation of lung function testing. Standardisation of spirometry. Eur Respir J 26:319–338
Armstrong BK, de Klerk NH, Musk AW, Hobbs MS (1988) Mortality in miners and millers of crocidolite in Western Australia. Br J Ind Med 45:5–13
Hansen J, de Klerk NH, Musk AW, Hobbs MS (1998) Environmental exposure to crocidolite and mesothelioma: exposure-response relationships. Am J Respir Crit Care Med 157:69–75
Kusaka Y, Hering KG (2005) International classification of HRCT for occupational and environmental respiratory diseases. Springer
Suganuma N, Kusaka Y, Hering KG et al (2009) Reliability of the proposed international classification of high-resolution computed tomography for occupational and environmental respiratory diseases. J Occup Health 51:210–222
Walsh SL, Calandriello L, Sverzellati N, Wells AU, Hansell DM, Consort UIPO (2016) Interobserver agreement for the ATS/ERS/JRS/ALAT criteria for a UIP pattern on CT. Thorax 71:45–51
Brantly M, Avila NA, Shotelersuk V, Lucero C, Huizing M, Gahl WA (2000) Pulmonary function and high-resolution CT findings in patients with an inherited form of pulmonary fibrosis, Hermansky-Pudlak syndrome, due to mutations in HPS-1. Chest 117:129–136
Diot E, Boissinot E, Asquier E et al (1998) Relationship between abnormalities on high-resolution CT and pulmonary function in systemic sclerosis. Chest 114:1623–1629
ILO (1980) International labour office. Guidelines for the use of ILO international classification of radiographs of pneumoconiosis. ILO, Geneva
Mastrangelo G, Ballarin MN, Bellini E et al (2009) Asbestos exposure and benign asbestos diseases in 772 formerly exposed workers: dose-response relationships. Am J Ind Med 52:596–602
Cookson WO, De Klerk NH, Musk AW, Armstrong BK, Glancy JJ, Hobbs MS (1986) Prevalence of radiographic asbestosis in crocidolite miners and millers at Wittenoom, Western Australia. Br J Ind Med 43:450–457
Tsushima K, Sone S, Yoshikawa S, Yokoyama T, Suzuki T, Kubo K (2010) The radiological patterns of interstitial change at an early phase: over a 4-year follow-up. Respir Med 104:1712–1721
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is A/Prof Fraser Brims.
Conflict of interest
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Funding
This study has received funding by the Western Australian Department of Health.
Statistics and biometry
One of the authors (Prof Nick de Klerk) has significant statistical expertise.
Ethical approval
Approval for the Asbestos Review Program was granted by the Western Australian Department of Health Human Research Ethics Committee, reference RA/4/1/2119.
Informed consent
Written informed consent was obtained from all subjects (patients) in this study.
Study subjects or cohorts overlap
Some study subjects or cohorts have been previously reported in: Murray CP, Wong PM, Teh J et al (2016) Ultra low dose CT screen-detected non-malignant incidental findings in the Western Australian Asbestos Review Programme. Respirology 21:1419-1424.
Methodology
Prospective, observational cohort study, performed at one institution.
Rights and permissions
About this article

Cite this article
Manners, D., Wong, P., Murray, C. et al. Correlation of ultra-low dose chest CT findings with physiologic measures of asbestosis. Eur Radiol 27, 3485–3490 (2017). https://doi.org/10.1007/s00330-016-4722-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-016-4722-7