
Abstract
Objectives
To assess the impact of clinically significant portal hypertension (CSPH) on the prognosis of patients with hepatocellular carcinoma (HCC) undergoing radiofrequency ablation (RFA).
Methods
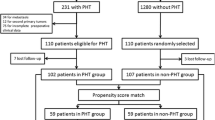
We retrospectively enrolled 280 treatment-naïve early-stage HCC patients who had Child–Pugh grade A or B and received upper gastrointestinal endoscopy at the time of HCC diagnosis. CSPH was defined as (1) a platelet count < 100,000/mm3 associated with splenomegaly and/or (2) the presence of oesophageal/gastric varices by endoscopy. Factors determining poor overall survival and recurrence after RFA were analysed by Cox proportional hazards model and propensity score matching analysis.
Results
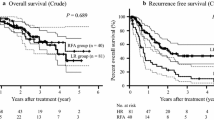
A total of 192 (68.6 %) patients had CSPH. The cumulative 5-year survival rates were 50.6 % and 76.7 % in patients with and without CSPH, respectively (p = 0.015). Based on multivariate analysis, age > 65 years (hazard ratio (HR) 1.740, p = 0.025), serum albumin levels ≤ 3.5 g/dL (HR 3.268, p < 0.001) and multiple tumours (HR 1.693, p = 0.046), but not CSPH, were independent risk factors associated with poor overall survival after RFA. Moreover, the overall survival rates were comparable between patients with and without CSPH after adjusting for confounding factors via propensity score matching analysis.
Conclusions
CSPH was not associated with poor outcomes after RFA.
Key points
• CSPH was common in HCC patients who underwent RFA therapy.
• CSPH was not an independent risk factor in determining poor prognosis.
• Serum albumin level was more important to determine the outcomes.



Similar content being viewed by others

Abbreviations
- AASLD:
-
American Association for the Study of Liver Disease
- AFP:
-
alpha-fetoprotein
- Alk-P:
-
alkaline phosphatase
- ALT:
-
alanine aminotransferase
- AST:
-
aspartate aminotransferase
- BCLC:
-
Barcelona Clinic Liver Cancer
- CI:
-
confidence interval
- CSPH:
-
clinically significant portal hypertension
- CT:
-
computed tomography
- EASL:
-
European Association for the Study of the Liver
- EGV:
-
oesophageal-gastric varix
- EV:
-
oesophageal varix
- GV:
-
gastric varix
- HBsAg:
-
hepatitis B surface antigen
- HBV:
-
hepatitis B virus
- HCC:
-
hepatocellular carcinoma
- HCV:
-
hepatitis C virus
- HR:
-
hazard ratio
- HVPG:
-
hepatic venous pressure gradient
- IRB:
-
Institutional review board
- MRI:
-
magnetic resonance imaging
- OS:
-
overall survival
- PH:
-
portal hypertension
- PT/INR:
-
prothrombin time/international ratio
- RFA:
-
radiofrequency ablation therapy
- RFS:
-
recurrence-free survival
- TACE:
-
transarterial chemoembolization
References
Bruix J, Sherman M (2011) Management of hepatocellular carcinoma: an update. Hepatology 53:1020–1022
de Lope CR, Tremosini S, Forner A, Reig M, Bruix J (2012) Management of HCC. J Hepatol 56(Suppl):S75–S87
Lin SM, Lin CJ, Lin CC, Hsu CW, Chen YC (2005) Randomised controlled trial comparing percutaneous radiofrequency thermal ablation, percutaneous ethanol injection, and percutaneous acetic acid injection to treat hepatocellular carcinoma of 3 cm or less. Gut 54:1151–1156
Lencioni R (2010) Loco-regional treatment of hepatocellular carcinoma. Hepatology 52:762–773
Livraghi T, Meloni F, Di Stasi M et al (2008) Sustained complete response and complications rates after radiofrequency ablation of very early hepatocellular carcinoma in cirrhosis: is resection still the treatment of choice? Hepatology 47:82–89
Hung HH, Chiou YY, Hsia CY et al (2011) Survival rates are comparable after radiofrequency ablation or surgery in patients with small hepatocellular carcinomas. Clin Gastroenterol Hepatol 9:79–86
Shiina S, Tateishi R, Arano T et al (2012) Radiofrequency ablation for hepatocellular carcinoma: 10-year outcome and prognostic factors. Am J Gastroenterol 107:569–577, quiz 578
Kao WY, Chiou YY, Hung HH et al (2012) Younger hepatocellular carcinoma patients have better prognosis after percutaneous radiofrequency ablation therapy. J Clin Gastroenterol 46:62–70
Kim YS, Lim HK, Rhim H et al (2013) Ten-year outcomes of percutaneous radiofrequency ablation as first-line therapy of early hepatocellular carcinoma: analysis of prognostic factors. J Hepatol 58:89–97
Seror O, N'Kontchou G, Nault JC et al (2016) Hepatocellular carcinoma within Milan criteria: no-touch multibipolar radiofrequency ablation for treatment-long-term results. Radiology. doi:10.1148/radiol.2016150743:150743
Fernandez M (2015) Molecular pathophysiology of portal hypertension. Hepatology 61:1406–1415
de Franchis R, Baveno VIF (2015) Expanding consensus in portal hypertension: report of the Baveno VI Consensus Workshop: stratifying risk and individualizing care for portal hypertension. J Hepatol 63:743–752
D'Amico G, Pasta L, Morabito A et al (2014) Competing risks and prognostic stages of cirrhosis: a 25-year inception cohort study of 494 patients. Aliment Pharmacol Ther 39:1180–1193
King LY, Canasto-Chibuque C, Johnson KB et al (2015) A genomic and clinical prognostic index for hepatitis C-related early-stage cirrhosis that predicts clinical deterioration. Gut 64:1296–1302
Fischer MA, Kartalis N, Grigoriadis A et al (2015) Perfusion computed tomography for detection of hepatocellular carcinoma in patients with liver cirrhosis. Eur Radiol 25:3123–3132
Bucci L, Garuti F, Camelli V et al (2016) Comparison between alcohol- and hepatitis C virus-related hepatocellular carcinoma: clinical presentation, treatment and outcome. Aliment Pharmacol Ther 43:385–399
Llovet JM, Fuster J, Bruix J (1999) Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology 30:1434–1440
Bruix J, Castells A, Bosch J et al (1996) Surgical resection of hepatocellular carcinoma in cirrhotic patients: prognostic value of preoperative portal pressure. Gastroenterology 111:1018–1022
Boleslawski E, Petrovai G, Truant S et al (2012) Hepatic venous pressure gradient in the assessment of portal hypertension before liver resection in patients with cirrhosis. Br J Surg 99:855–863
Cucchetti A, Cescon M, Golfieri R et al (2016) Hepatic venous pressure gradient in the preoperative assessment of patients with resectable hepatocellular carcinoma. J Hepatol 64:79–86
European Association For The Study Of The L, European Organisation for Research and Treatment of Cancer (2012) EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 56:908–943
Bruix J, Reig M, Sherman M (2016) Evidence-based diagnosis, staging, and treatment of patients with hepatocellular carcinoma. Gastroenterology 150:835–853
Bruix J, Sherman M, Llovet JM et al (2001) Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL Conference. J Hepatol 35:421–430
Su CW, Chau GY, Hung HH et al (2015) Impact of steatosis on prognosis of patients with early-stage hepatocellular carcinoma after hepatic resection. Ann Surg Oncol 22:2253–2261
D'Agostino RB Jr (1998) Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat Med 17:2265–2281
Ishizawa T, Hasegawa K, Aoki T et al (2008) Neither multiple tumors nor portal hypertension are surgical contraindications for hepatocellular carcinoma. Gastroenterology 134:1908–1916
Roayaie S, Jibara G, Tabrizian P et al (2015) The role of hepatic resection in the treatment of hepatocellular cancer. Hepatology 62:440–451
Santambrogio R, Kluger MD, Costa M et al (2013) Hepatic resection for hepatocellular carcinoma in patients with Child–Pugh's A cirrhosis: is clinical evidence of portal hypertension a contraindication? HPB (Oxford) 15:78–84
Berzigotti A, Reig M, Abraldes JG, Bosch J, Bruix J (2015) Portal hypertension and the outcome of surgery for hepatocellular carcinoma in compensated cirrhosis: a systematic review and meta-analysis. Hepatology 61:526–536
Nault JC, De Reynies A, Villanueva A et al (2013) A hepatocellular carcinoma 5-gene score associated with survival of patients after liver resection. Gastroenterology 145:176–187
Wu WC, Chiou YY, Hung HH et al (2012) Prognostic significance of computed tomography scan-derived splenic volume in hepatocellular carcinoma treated with radiofrequency ablation. J Clin Gastroenterol 46:789–795
Ding Y, Rao SX, Chen C, Li R, Zeng MS (2015) Assessing liver function in patients with HBV-related HCC: a comparison of T(1) mapping on Gd-EOB-DTPA-enhanced MR imaging with DWI. Eur Radiol 25:1392–1398
Lee DH, Lee JM, Lee JY et al (2014) Radiofrequency ablation of hepatocellular carcinoma as first-line treatment: long-term results and prognostic factors in 162 patients with cirrhosis. Radiology 270:900–909
Garcia-Tsao G, Bosch J (2015) Varices and variceal hemorrhage in cirrhosis: a new view of an old problem. Clin Gastroenterol Hepatol 13:2109–2117
Lee TY, Lin JT, Zeng YS, Chen YJ, Wu MS, Wu CY (2015) Association between nucleos(t)ide analogue and tumor recurrence in HBV-related hepatocellular carcinoma after radiofrequency ablation. Hepatology. doi:10.1002/hep.28266
Reig M, Marino Z, Perello C et al (2016) Unexpected early tumor recurrence in patients with hepatitis C virus -related hepatocellular carcinoma undergoing interferon-free therapy: a note of caution. J Hepatol. doi:10.1016/j.jhep.2016.04.008
Marcellin P, Gane E, Buti M et al (2013) Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year open-label follow-up study. Lancet 381:468–475
Hosaka T, Suzuki F, Kobayashi M et al (2013) Long-term entecavir treatment reduces hepatocellular carcinoma incidence in patients with hepatitis B virus infection. Hepatology 58:98–107
Acknowledgments
The authors thank American Manuscript Editors for English editing and writing assistance. This work was supported by grants from the National Science Council of Taiwan (NSC 101-2314-B-075-013-MY2), Ministry of Science and Technology of Taiwan (MOST 103-2314-B-075-077, and 104-2314-B-075-076), grants from Taipei Veterans General Hospital (V102C-117 and V104-111), a grant from the Ministry of Education Aim for the Top University Plan (103 AC-T402) and a grant from the Center of Excellence for Cancer Research at TVGH (MOHW104-TDU-B-211-124-001) in Taipei, Taiwan. We also thank for the Clinical Research Core Laboratory of Taipei Veterans General Hospital for providing experimental space and facilities. We thank Pui-Ching Lee for kindly providing statistical advice for this manuscript. Yi-You Chiou is the guarantor for the entire study. The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article. Institutional review board approval was obtained. Written informed consent was obtained from all subjects (patients) in this study. Some study subjects or cohorts have been previously reported in an oral presentation at the 23rd United European Gastroenterology Week in 2015. Methodology: retrospective, observational, performed at one institution.
Author information
Authors and Affiliations
Corresponding author
Additional information
Kuan-Chieh Fang and Chien-Wei Su contributed equally to this work.
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOCX 28 kb)
Fig. S1
Cumulative curves of OS rates in HCC patients after RFA stratified by CSPH status and serum albumin levels. Patients with serum albumin levels > 3.5 g/dL had a higher OS rate than their counterparts among both patients with CSPH (S1A, p = 0.003) and patients without CSPH (S1B, p = 0.006). (GIF 49 kb)
(GIF 47 kb)
Fig. S2
Cumulative curves of OS rates after RFA in patients with BCCL stage 0 HCC stratified by CSPH status and serum albumin levels. Patients with serum albumin levels > 3.5 g/dL had a higher OS rate than their counterparts among all patients (S1A, p < 0.001), among patients with CSPH (S1B, p < 0.001) and among patients without CSPH (S1C, p = 0.010). (GIF 46 kb)
(GIF 42 kb)
(GIF 39 kb)
Fig. S3
Cumulative RFS curves after RFA for patients with HCC stratified by CSPH. A. The cumulative RFS rates were similar between patients with and without CSPH both before (S3A, p = 0.575) and after propensity score matching analysis (S3B, p = 0.856). In addition, for patients with BCLC stage 0 HCC, the RFS rates were also comparable between the two groups of patients (S3C, p = 0.719). (GIF 352 kb)
(GIF 66 kb)
(GIF 81 kb)
Rights and permissions
About this article

Cite this article
Fang, KC., Su, CW., Chiou, YY. et al. The impact of clinically significant portal hypertension on the prognosis of patients with hepatocellular carcinoma after radiofrequency ablation: a propensity score matching analysis. Eur Radiol 27, 2600–2609 (2017). https://doi.org/10.1007/s00330-016-4604-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-016-4604-z