
Abstract
Purpose
Neither the performance of CT in diagnosing penetrating gastrointestinal injury nor its ability to discriminate patients requiring either observation or surgery has been determined.
Materials and methods
This was a prospective, single-institutional observational study of patients with penetrating injury to the torso who underwent CT. Based on CT signs, reviewers determined the presence of a gastrointestinal injury and the need for surgery or observation. The primary outcome measures were operative findings and clinical follow-up. CT results were compared with the primary outcome measures.
Results
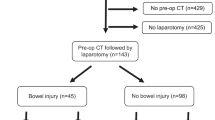
Of one hundred and seventy-one patients (72 gunshot wounds, 99 stab wounds; age range, 18–57 years; median age, 28 years) with penetrating torso trauma who underwent CT, 45 % were followed by an operation and 55 % by clinical follow up. Thirty-five patients had a gastrointestinal injury at surgery. The sensitivity, specificity, and accuracy of CT for diagnosing a gastrointestinal injury for all patients were each 91 %, and for predicting the need for surgery, they were 94 %, 93 %, 93 %, respectively. Among the 3 % of patients who failed observation, 1 % had a gastrointestinal injury.
Conclusion
CT is a useful technique to diagnose gastrointestinal injury following penetrating torso injury. CT can help discriminate patients requiring observation or surgery.
Key Points
• The most sensitive sign is wound tract extending up to gastrointestinal wall.
• The most accurate sign is gastrointestinal wall thickening.
• Triple-contrast CT is a useful technique to diagnose gastrointestinal injury.
• Triple-contrast CT helps to discriminate patients requiring observation and surgery.




Similar content being viewed by others

References
Como JJ, Bokhari F, Chiu WC et al (2010) Practice management guidelines for selective nonoperative management of penetrating abdominal trauma. J Trauma 68:721–733
Inaba K, Okoye OT, Rosenheck R et al (2013) Prospective evaluation of the role of computed tomography in the assessment of abdominal stab wounds. JAMA Surg 148:810–816
Biffl WL, Kaups KL, Cothren CC et al (2009) Management of patients with anterior abdominal stab wounds: a Western Trauma Association multicenter trial. J Trauma 66:1294–1301
Plackett TP, Fleurat J, Putty B, Demetriades D, Plurad D (2011) Selective nonoperative management of anterior abdominal stab wounds: 1992–2008. J Trauma 70:408–413, discussion 413–414
Jansen JO, Inaba K, Resnick S (2013) Selective non-operative management of abdominal gunshot wounds: survey of practise. Injury 44:639–644
Phillip T, Sclafani SJ, Goldstein A, Scalea T, Panetta T, Shaftan G (1986) Use of the contrast-enhanced CT enema in the management of penetrating trauma to the flank and back. J Trauma 26:593–601
Shanmuganathan K, Mirvis SE, Chiu WC, Killeen KL, Hogan GJ, Scalea TM (2004) Penetrating torso trauma: triple-contrast helical CT inperitoneal violation and organ injury—a prospective study in 200 patients. Radiology 231:775–778
Munera F, Morales C, Soto JA et al (2004) Gunshot wounds of abdomen: evaluation of stable patients with triple-contrast helical CT. Radiology 231:399–405
Fakhry SM, Brownstein M, Watts DD, Baker CC, Oller D (2000) Relatively short diagnostic delays (<8 hours) produce morbidity and mortality in blunt small bowel injury: an analysis of time to operative intervention in 198 patients from a multicenter experience. J Trauma 48:408–414, discussion 414–415
Inaba K, Branco BC, Moe D et al (2012) Prospective evaluation of selective nonoperative management of torso gunshot wounds: when is it safe to discharge? J Trauma Acute Care Surg 72:884–891
Biffl WL, Kaups KL, Pham TN et al (2011) Validating the Western Trauma Association algorithm for managing patients with anterior abdominal stab wounds: a Western Trauma Association multicenter trial. J Trauma 71:1494–1502
Hosmer DW, Lemeshow S, Sturdivant RX (2013) Applied logistic regression, 3rd edn. Wiley, New York
Hastie T, Tibshirani R, Friedman J (2009) The elements of statistical learning: data mining, inference, and prediction, 2nd edn. Springer, New York
Hayes AF, Krippendorff K (2007) Answering the Call for a Standard Reliability Measure for Coding Data. Commun Methods Measures 1:77–89
Shaftan GW (1960) Indications for operation in abdominal trauma. Am J Surg 99:657–664
Feliciano DV, Bitonodo CG, Steed G, Mattox KL, Burch JM, Jordan GL Jr (1984) Five hundred open taps or lavages in patients with abdominal stab wounds. Ann J Surg 147:772–777
Demetriades D, Rabinowitz B (1987) Indications for operation in abdominal stab wounds. A prospective study of 651 patients. Ann Surg 203:129–132
Uranues S, Popa DE, Diaconescu B, Schrittwieser R (2015) Laparoscopy in penetrating abdominal trauma. World J Surg 39:1381–1388
Leppäniemi A, Haapiainen R (2003) Diagnostic laparoscopy in abdominal stab wounds: a prospective, randomized study. J Trauma 55:636–645
Renz BM, Feliciano DV (1995) Unnecessary laparotomies for trauma: a prospective study of morbidity. J Trauma 38:350–356
Haan J, Kole K, Brunetti A, Kramer M, Scalea TM (2003) Nontherapeutic laparotomies revisited. Am Surg 69:562–565
Acknowledgements
The scientific guarantors of this publication are Kathirkamanathan Shanmuganathan & Nitima Saksobhavivat. The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
The authors state that this work has not received any funding. One of the authors has significant statistical expertise. Institutional review board approval was obtained. Written informed consent was waived by the institutional review board. Methodology: prospective, observational, performed at one institution.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Saksobhavivat, N., Shanmuganathan, K., Boscak, A.R. et al. Diagnostic accuracy of triple-contrast multi-detector computed tomography for detection of penetrating gastrointestinal injury: a prospective study. Eur Radiol 26, 4107–4120 (2016). https://doi.org/10.1007/s00330-016-4260-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-016-4260-3