
Abstract
Objectives
The purpose of this study was to determine whether performing the test bolus (TB) of computed tomography coronary angiography (CTCA) and computed tomography pulmonary angiography (CTPA) at 80 kVp reduces dose without compromising diagnostic quality.
Methods
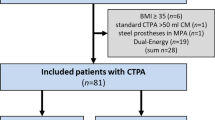
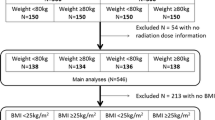
An 80 kVp TB protocol for CTCA and CTPA was retrospectively compared to standard TB protocol (non-obese: 100 kVp, obese: 120 kVp). CT angiogram parameters were unchanged between cohorts. Thirty-seven consecutive 80 kVp TB CTCA images were compared to 53 standard CTCA images. Fifty consecutive CTPAs from each protocol were analysed. Diagnostic quality of the CT angiogram was assessed by: mean attenuation, signal-to-noise ratio (SNR) in the ascending aorta (AA) in CTCA and in the main pulmonary artery (MPA) in CTPA, diagnostic rate, and number of repeated monitoring scans. Mean effective dose was estimated using the dose-length product.
Results
Mean TB effective doses were significantly lower (P < 0.0001) for 80 kVp scans compared to the standard in non-obese CTCA (0.15 ± 0.04 mSv Vs 0.33 ± 0.09 mSv), obese CTCA (0.17 ± 0.06 mSv Vs 0.57 ± 0.12 mSv), and CTPA patients (0.07 ± 0.03 mSv Vs 0.15 ± 0.06 mSv). No difference was demonstrated in mean attenuation, SNR (AA), SNR (MPA), diagnostic rates, or number of repeated monitoring scans between protocols.
Conclusions
Routinely performing TB at 80 kVp, regardless of body habitus, in CTCA and CTPA results in a small but significant dose reduction, without compromising CT angiogram diagnostic quality.
Key Points
• CT coronary angiography is performed to exclude the presence of significant coronary atherosclerosis.
• CT pulmonary angiography is performed to diagnose pulmonary thromboembolism.
• This retrospective study showed dose reduction by performing test bolus at 80 kVp.
• Diagnosis can be made with reduced exposure to ionising radiation.


Similar content being viewed by others

Abbreviations
- CTCA:
-
CT coronary angiography
- CTPA:
-
CT pulmonary angiography
- CAD:
-
Coronary artery disease
- PE:
-
Pulmonary embolism
- TB:
-
Test bolus
- BMI:
-
Body mass index
- AA:
-
Ascending aorta
- MPA:
-
Main pulmonary artery
- ROI:
-
Region of interest
- DLP:
-
Dose length product
- CTDIvol :
-
Volume computed tomography dose index
- ED:
-
Effective dose
- SNR:
-
Signal-to-noise ratio
- IN:
-
Image noise
- ICC:
-
Intraclass correlation coefficient
- IRMER 2000:
-
Ionising Radiation (Medical Exposure) Regulations 2000
References
(2010) Chest pain of recent onset: assessment and investigation of recent onset chest pain or discomfort of suspected cardiac origin. NICE guideline: CG95
Rodrigues JC, Mathias H, Negus IS, Manghat NE, Hamilton MC (2012) Intravenous contrast medium administration at 128 multi-detector row CT pulmonary angiography: bolus tracking versus test bolus and the implications for diagnostic quality and effective dose. Clin Radiol 67:1053–1060
Gosling O, Morgan-Hughes G, Iyengar S et al (2013) Computed tomography to diagnose coronary artery disease: a reduction in radiation dose increases applicability. Clin Radiol 68:340–345
Bjorkdahl P, Nyman U (2010) Using 100- instead of 120-kVp computed tomography to diagnose pulmonary embolism almost halves the radiation dose with preserved diagnostic quality. Acta Radiol 51:260–270
Health Protection Agency (2009). Defining Research. Health Protection Agency, United Kingdom. Available via http://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1272032326180. Accessed 5 May 2012
Stolzmann P, Scheffel H, Schertler T et al (2008) Radiation dose estimated in dual-source computed tomography coronary angiography. Eur Radiol 18:592–599
Bongartz G, Golding SJ, Jurik AG et al. (2000) European Guidelines on quality criteria for computed tomography. EUR 16262 EN. European Commission
Gosling O, Loader R, Venables P, Rowles N, Morgan-Hughes G, Roobottom C (2010) Cardiac CT: are we underestimating the dose? A radiation dose study utilizing the 2007 ICRP tissue weighting factors and a cardiac specific scan volume. Clin Radiol 65:1013–1017
Huda W, Ogden KM, Khorasani MR (2008) Converting dose length product to effect dose at CT. Radiology 248:995–1003
Jones DG, Shrimpton PC (1993) NRPB-SR 250: Normalised organ doses for x-ray computed tomography calculated using monte carlo techniques. Health Protection Agency, United Kingdom. Available via http://www.hpa.org.uk/web/HPAweb&HPAwedStandard/HPAweb_C/1195733753330. Accessed 3 Nov 2013
Mortimer AM, Singh RK, Hughes J, Greenwood R, Hamilton MC (2011) Use of expiratory CT pulmonary angiography to reduce inspiration and breath-hold associated artefact: contrast dynamics and implications for scan protocol. Clin Radiol 66:1159–1166
Henk CB, Grampp S, Linnau KF et al (2003) Suspected pulmonary embolism: enhancement of pulmonary arteries at deep inspiration CT angiography – influence of patent foramen ovale and atrial-septal defect. Radiology 226:749–755
Bellenger NG, Davies LC, Francis JM, Coats AJ, Pennell DJ (2000) Reduction in sample size for studies of remodelling in heart failure by the use of cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2:271–278
United Kingdom Government legislation (2000). The Ionising Radiation (Medical Exposure) Regulations 2000. United Kingdom Government, United Kingdom. Available via http://www.legislation.gov.uk/uksi/2000/1059/contents/made. Accessed 5 May 2012
Chem MY, Steigner ML, Leung SW et al (2013) Simulated 50 % radiation dose reduction in coronary CT angiography using adaptive iterative dose reduction in three-dimensions (AIDR3D). Int J Cardiovasc Imaging 29:1167–1175
Acknowledgments
This work was conducted in conjunction with the National Institute for Health Research (NHIR) Biomedical Research Unit at The Bristol Heart Institute. The work does not necessarily reflect the opinion of the NIHR.
The scientific guarantor of this publication is Dr Mark Hamilton. The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. The authors state that this work has not received any funding. No complex statistical methods were necessary for this paper. Institutional Review Board approval was not required because this retrospective evaluation of clinical service delivery does not require Research Ethics Committee review, in accordance with the National Health Service Research Ethics Service guidelines. Written informed consent was not required for this study because this retrospective evaluation of clinical service delivery does not require Research Ethics Committee review, in accordance with the National Health Service Research Ethics Service guidelines. Approval from the institutional animal care committee was not required because this study did not involve animals.
Methodology: retrospective, case-control study, performed at one institution.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Rodrigues, J.C.L., Joshi, D., Lyen, S.M. et al. Tube potential can be lowered to 80 kVp in test bolus phase of CT coronary angiography (CTCA) and CT pulmonary angiography (CTPA) to save dose without compromising diagnostic quality. Eur Radiol 24, 2458–2466 (2014). https://doi.org/10.1007/s00330-014-3281-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-014-3281-z