
Abstract
Objectives
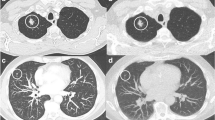
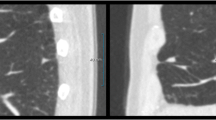
To assess the long-term stability of small (<10 mm) non-calcified pulmonary nodules (NCNs) in high-risk subjects initially screened for lung cancer using low-dose chest computed tomography (LDCCT).
Methods
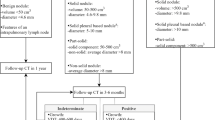
A total of 449 subjects initially underwent screening with serial LDCCT over a 2-year period. Participants identified as having NCNs ≥10 mm were referred for formal lung cancer workup. NCNs <10 mm diameter were followed in accordance with the study protocol. Seven years after baseline screening, subjects with previously documented NCNs <10 mm, which were unchanged in size after the 2-year follow-up period, were re-imaged using LDCCT to assess for interval nodule growth.
Results
Eighty-three subjects with previously documented stable NCNs <10 mm underwent LDCCT at 7 years. NCNs were unchanged in 78 subjects and had decreased in size in 4 subjects. There was interval growth of an NCN (from 6 mm to 9 mm) in one subject re-imaged at 7 years, but this nodule has remained stable in size over a further 2-year follow-up period.
Conclusions
Non-calcified pulmonary nodules <10 mm in size that are unchanged in size or smaller after 2 years of follow-up with LDCCT are most likely benign.
Key Points
• Computed tomography is increasingly used for screening for lung cancer.
• However CT frequently reveals unsuspected lung nodules.
• Seven-year follow-up of small (<10 mm) non-calcified pulmonary nodules is reassuring.
• Even in high-risk patients most nodules will likely be benign.

Similar content being viewed by others
References
Shibuya K, Mathers CD, Boschi-Pinto C, Lopez AD, Murray CJ (2002) Global and regional estimates of cancer mortality and incidence by site: II. Results for the global burden of disease 2000. BMC Cancer 2:37
Henschke CI, McCauley DI, Yankelevitz DF et al (1999) Early Lung Cancer Action Project: overall design and findings from baseline screening. Lancet 354:99–105
Byrne AL, Logan PM (2006) Screening for lung cancer. Radiol Updat 5:85–91
Sobue T, Moriyama N, Kaneko M et al (2002) Screening for lung cancer with low-dose helical computed tomography: anti-lung cancer association project. J Clin Oncol 20:911–920
Henschke CI, Naidich DP, Yankelevitz DF et al (2001) Early lung cancer action project: initial findings on repeat screenings. Cancer 92:153–159
Noguchi M, Morikawa A, Kawasaki M et al (1995) Small adenocarcinoma of the lung. Histologic characteristics and prognosis. Cancer 75:2844–2852
Aberle DR, Adams AM, Berg CD et al (2011) Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 365:395–409
Macredmond R, Logan PM, Lee MJ, Kenny D, Foley C, Costello RW (2004) Screening for lung cancer using low dose CT scanning. Thorax 59:237–241
Macredmond R, McVey G, Lee MJ et al (2006) Screening for lung cancer using low dose CT scanning: results of 2 year follow up. Thorax 61:54–56
Wahidi MM, Govert JA, Goudar RK, Gould MK, McCrory DC (2007) Evidence for the treatment of patients with pulmonary nodules: when is it lung cancer?: ACCP evidence-based clinical practice guidelines (2nd edition). Chest 132:94S–107S
Edey AJ, Hansell DM (2009) Incidentally detected small pulmonary nodules on CT. Clin Radiol 64:872–884
MacMahon H, Austin JH, Gamsu G et al (2005) Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology 237:395–400
Khan A (2007) ACR Appropriateness Criteria on solitary pulmonary nodule. J Am Coll Radiol 4:152–155
Gould MK, Fletcher J, Iannettoni MD et al (2007) Evaluation of patients with pulmonary nodules: when is it lung cancer?: ACCP evidence-based clinical practice guidelines (2nd edition). Chest 132:108S–130S
Good CA, Wilson TW (1958) The solitary circumscribed pulmonary nodule; study of seven hundred five cases encountered roentgenologically in a period of three and one-half years. J Am Med Assoc 166:210–215
Good CA (1953) Management of patient with solitary mass in lung. Chic Med Soc Bull 55:893–896
Good CA, Hood RT Jr, Mc DJ (1953) Significance of a solitary mass in the lung. Am J Roentgenol Radium Ther Nucl Med 70:543–554
Hood RT Jr, Good CA, Clagett OT, McDonald JR (1953) Solitary circumscribed lesions of the lung; study of 156 cases in which resection was performed. J Am Med Assoc 152:1185–1191
Yankelevitz DF, Henschke CI (1997) Does 2-year stability imply that pulmonary nodules are benign? AJR Am J Roentgenol 168:325–328
Lillington GA (1991) Management of solitary pulmonary nodules. Dis Mon 37:271–318
Winer-Muram HT, Jennings SG, Tarver RD et al (2002) Volumetric growth rate of stage I lung cancer prior to treatment: serial CT scanning. Radiology 223:798–805
Revel MP, Merlin A, Peyrard S et al (2006) Software volumetric evaluation of doubling times for differentiating benign versus malignant pulmonary nodules. AJR Am J Roentgenol 187:135–142
Yankelevitz DF, Reeves AP, Kostis WJ, Zhao B, Henschke CI (2000) Small pulmonary nodules: volumetrically determined growth rates based on CT evaluation. Radiology 217:251–256
Quint LE, Cheng J, Schipper M, Chang AC, Kalemkerian G (2008) Lung lesion doubling times: values and variability based on method of volume determination. Clin Radiol 63:41–48
Hasegawa M, Sone S, Takashima S et al (2000) Growth rate of small lung cancers detected on mass CT screening. Br J Radiol 73:1252–1259
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Slattery, M.M., Foley, C., Kenny, D. et al. Long-term follow-up of non-calcified pulmonary nodules (<10 mm) identified during low-dose CT screening for lung cancer. Eur Radiol 22, 1923–1928 (2012). https://doi.org/10.1007/s00330-012-2443-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-012-2443-0