
Abstract
Purpose: To clarify the limitations of transcatheter treatment for hepatocellular carcinoma (HCC) with parasitic feeders from the cystic artery.
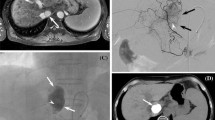
Methods: Three male patients had a solitary HCC (average diameter 3 cm) fed by the cystic artery among 221 patients with HCC from 1994 to 1997. One tumor was nourished entirely from the cystic artery arising from the medial branch of the left hepatic artery, and two tumors were fed partially by the cystic arteries arising from the anterior inferior branch of the right hepatic artery. We analyzed the indications for transcatheter treatment for these three patients.
Results: We chose not to embolize the cystic artery for fear of necrosis of the gallbladder. Although embolization of the anterior branch of the right hepatic artery was performed in one patient with a tumor fed partially by the cystic artery, only half the tumor was embolized. Two patients underwent hepatic resection, and one received percutaneous ethanol injection therapy. At follow-up of 28–40 months (average 33 months) all patients are alive.
Conclusion: Feeding by the cystic artery represents a limitation of TAE for HCC.
Similar content being viewed by others


References
Yamasaki S, Makuuchi M, Hasegawa H (1991) Results of hepatectomy for hepatocellular carcinoma at the National Cancer Center Hospital. HPB Surg 3:235–249
Yamada R, Kishi K, Sonomura T, Tsuda M, Nomura S, Satoh M (1990) Transcatheter arterial embolization in unresectable hepatocellular carcinoma. Cardiovasc Intervent Radiol 13:135–139
Ohishi H, Uchida H, Yoshimura H, Ohue S, Ueda J, Katsurag M, Matsuo N, Hosogi Y (1985) Hepatocellular carcinoma detected by iodized oil: Use of anticancer agents. Radiology 154:25–29
Lencioni R, Pinto F, Armillotta N, Bassi AM, Moretti M, Di-Giulio M, Marchi S, Uliana M, Della-Capanna S, Lencioni M, Bartolozzi C (1997) Long-term results of percutaneous ethanol injection therapy for hepatocellular carcinoma in cirrhosis: A European experience. Eur Radiol 7:514–519
Sato M, Watanabe Y, Ueda S, Iseki S, Abe Y, Sato N, Kimura S, Okubo K, Onji M (1996) Microwave coagulation therapy for hepatocellular carcinoma. Gastroenterology 110:1507–1514
Simons RK, Sinanan MN, Coldwell DM (1992) Gangrenous cholecytitis as a complication of hepatic artery embolization. Surgery 112:106–110
Takayasu K, Moriyama N, Muramatsu Y, Shima Y, Ushio K, Yamada T, Kishi K, Hasegawa H (1985) Gallbladder infarction after hepatic artery embolization. AJR 144:135–138
Nakarnura H, Kodoh H (1986) Emphysematous cholecystitis: Complication of hepatic artery embolization. Cardiovasc Intervent Radiol 9:152–153
Akamatsu K, Miyauchi S, Oshima K, Okita S, Yasuhara Y, Mogami H, Ohta Y, Hamamoto K (1989) Alleviation of gallbladder complication by treatment of hepatic arterial embolization with caerulein. Cancer Chemother Pharmacol [Suppl] 23:S59-S64
Daseler EH, Anson BJ, Hambley WC, Reiman AF (1947) The cystic artery and constituents of the hepatic pedicle. Surg Gynecol Obstet 85:47–63
Vandamme JPJ, Bonte J, van der Schueren G (1969) A reevaluation of hepatic and cystic arteries: The importance of the hepatic branches. Acta Anat 73:192–209
Price P, Holden C (1993) Anatomic variance in the cholecystic blood supply: A case report. Am Surg 59:278–280
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Hirota, S., Matsumoto, S., Fukuda, T. et al. Solitary hepatocellular carcinoma fed by the cystic artery: Limitation of transcatheter arterial embolization. Cardiovasc Intervent Radiol 22, 206–209 (1999). https://doi.org/10.1007/s002709900367
Issue Date:
DOI: https://doi.org/10.1007/s002709900367