
Abstract
Purpose
Complete biliary occlusions at different anatomic locations that are not amenable to surgical, endoscopic, or routine percutaneous methods pose a challenge to physicians. Biliary ductal neoanastomosis technique can play a very important role in solving such clinical problems.
Materials
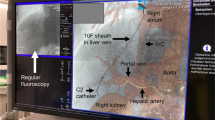
Between October 2004 and January 2018, six patients were treated in our institution for biliary drainage using biliary ductal neoanastomosis technique via sharp recanalization and a staged approach to achieve internal/external biliary drainage. All procedures were performed in an angiography suite by an interventional radiologist after multidisciplinary discussion.
Results
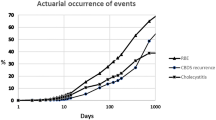
The mean patient age of the cohort was 54 years and 50% of the patients were female (three/six patients). The cause of obstruction was complications or disease progression after Whipple procedure in four patients, partial hepatectomy in one patient and benign biliary stricture after radioembolization in one patient. All patients were treated with percutaneous biliary neoanastomosis. All procedures were successfully performed in all six patients (100% technical success) without any major complications. All patients were successfully managed by capped drainage catheters for the duration of the follow up (one patient was transitioned to endoscopically inserted biliary stent, and in one patient the tube was eventually removed after establishment of patent neoanastomosis).
Conclusions
Biliary ductal neoanastomosis is an effective treatment option when the anatomy has been significantly altered in the post-surgical setting and wire cannot be safely passed into target draining organ or the remainder of biliary system. When performed by an experienced operator, this technique is safe and effective with a high technical success rate.




Similar content being viewed by others

References
Bricault I. Biliary obstruction: not always simple! Diagn Interv Imaging. 2013;94(7–8):729–40.
Choi SH, Han JK, Lee JM, et al. Differentiating malignant from benign common bile duct stricture with multiphasic helical CT. Radiology. 2005;236(1):178–83.
Jablonska B, Lampe P. Iatrogenic bile duct injuries: etiology, diagnosis and management. World J Gastroenterol. 2009;15(33):4097–104.
Pellegrini CA, Thomas MJ, Way LW (1984) Recurrent biliary stricture. Patterns of recurrence and outcome of surgical therapy. Am J Surg, 147(1):175–180
Genest JF, Nanos E, Grundfest-Broniatowski S, Vogt D, Hermann RE. Benign biliary strictures: an analytic review (1970 to 1984). Surgery. 1986;99(4):409–13.
McCarthy CJ, Thabet A, Yamada K, Mueller PR, Vagefi PA. Percutaneous creation of biliary-enteric neoanastomosis for anastomotic biliary occlusion following living donor liver transplantation. Liver Transpl. 2017;23(2):262–5.
Shlansky-Goldberg RD, Ginsberg GG, Cope C. Percutaneous puncture of the common bile duct as a rendezvous procedure to cross a difficult biliary obstruction. J Vasc Interv Radiol. 1995;6(6):943–6.
Salerno R, Davies SEC, Mezzina N, Ardizzone S. Comprehensive review on EUS-guided biliary drainage. World J Gastrointest Endosc. 2019;11(5):354–64.
De Robertis R, Contro A, Zamboni G, Mansueto G. Totally percutaneous rendezvous techniques for the treatment of bile strictures and leakages. J Vasc Interv Radiol. 2014;25(4):650–4.
Soulez G, Gagner M, Therasse E, et al. Malignant biliary obstruction: preliminary results of palliative treatment with hepaticogastrostomy under fluoroscopic, endoscopic, and laparoscopic guidance. Radiology. 1994;192(1):241–6.
Soulez G, Therasse E, Oliva VL, et al. Left hepaticogastrostomy for biliary obstruction: long-term results. Radiology. 1997;204(3):780–6.
Ito K, Ogawa T, Horaguchi J, Koshita S, Fujita N. Reintervention for occluded biliary metal stent for patients with malignant distal biliary stricture. Dig Endosc. 2013;25(Suppl 2):126–31.
Tipaldi L. A simplified percutaneous hepatogastric drainage technique for malignant biliary obstruction. Cardiovasc Intervent Radiol. 1995;18(5):333–6.
Mistry JH, Varma V, Mehta N, Kumaran V, Nundy S, Gupta A. Percutaneous transhepatic hepaticogastrostomy for portal biliopathy: a novel approach. Trop Gastroenterol. 2012;33(2):140–3.
Ozkan OS, Akinci D, Abbasoglu O, Karcaaltincaba M, Ozmen MN, Akhan O. Percutaneous hepaticogastrostomy in a patient with complete common duct obstruction after right hepatectomy. J Vasc Interv Radiol. 2005;16(9):1253–6.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors declare that they do not have any conflict of interest.
Ethical Approval
Institutional review board approval for anonymous retrospective review of patients and informed consent is not required at our institution.
Informed Consent
All authors consent for the publication of the current article in the Cardiovascular and Interventional Radiology.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Habibollahi, P., Benjamin, J.L., X. Bai, H. et al. Percutaneous Fluoroscopic-Guided Creation of Neoanastomosis for the Treatment of Biliary Occlusions. Cardiovasc Intervent Radiol 43, 1671–1678 (2020). https://doi.org/10.1007/s00270-020-02544-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-020-02544-z