
Abstract
Background
Uterine fibroid embolisation (UFE) is an effective treatment for fibroids. There are varying analgesia protocols published to control procedure associated pain. We aimed to assess what protocols are most effective in controlling post-procedural pain.
Materials and Methods
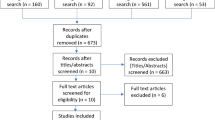
A systematic review of the Embase and Medline databases was conducted according to PRISMA guidelines. Studies regarding analgesia protocols post-uterine fibroid embolisation with Visual Analogue Scale or Numerical Rating Scale pain scores were included. The mean maximal pain scores of patients post-procedure were evaluated. ANOVA and t tests were performed.
Results
We identified 26 studies (total 3353 patients), with a mean procedural success rate of > 87%. We stratified protocols into four groups. Mean pain scores were: opioids ± NSAIDs ± acetaminophen (4.84, SD = 1.56); opioids ± NSAIDs ± acetaminophen + nerve block (4.7, SD = 1.37); opioids ± NSAIDs ± acetaminophen + intrauterine artery drug administration (4.09, SD = 0.60); and opioids ± NSAIDs ± acetaminophen + other (5.30, SD = 1.13) without significant difference between groups (p = 0.71). Similarly, there was no difference (p = 0.057) between groups for time to discharge or side effects.
Conclusions
There is no evidence to suggest that there is any superiority of one protocol above another in the published literature. Appropriate use of opioids ± NSAIDs ± acetaminophen alone appears to be sufficient to control pain post-UFE. However, due to large heterogeneity of the literature no firm conclusions can be reached, and further research is warranted.
Level of Evidence
Level 1, Systematic review.

Similar content being viewed by others


References
Fujii S, et al. Fibroids: basic science and etiology. Int Congr Ser. 2004;1266:183–90.
Ravina JH, Ciraru-Vigneron N, Bouret JM, Herbreteau D, Houdart E, Aymard A, Merland JJ. Arterial embolisation to treat uterine myomata. Lancet. 1995;364:671–2.
Gupta JK, Sinha A, Lumsden MA, Hickey M. Uterine artery embolization for symptomatic uterine fibroids. Cochrane Database Syst Rev. 2014. https://doi.org/10.1002/14651858.CD005073.pub4.
Bilhim T, Pisco JM. The role of nonsteroidal anti-inflammatory drugs (NSAIDS) in the management of the post-embolization symptoms after uterine artery embolization. Pharmaceuticals. 2010;3:1729–38.
Lipszyc M, Winters E, Engelman E, Baurain M, Barvais L. Remifentanil patient-controlled analgesia effect-site target-controlled infusion compared with morphine patient-controlled analgesia for treatment of acute pain after uterine artery embolization. Br J Anaesth. 2011;106:724–31.
Siskin GP, Stainken BF, Dowling K, Meo P, Ahn J, Dolen EG. Outpatient uterine artery embolization for symptomatic uterine fibroids: experience in 49 patients. J Vasc Interv Radiol. 2000;11:305–11.
Nemcek AA, Sichlau M, Vogelzang R. Comparison of pain after uterine artery embolization using tris-acryl gelatin microspheres versus polyvinyl alcohol particles. Cardiovasc Intervent Radiol. 2004;26:375–8.
Katsumori T, Arima H, Asai S, Hayashi N, Miura H. Comparison of pain within 24 h after uterine artery embolization with tris-acryl gelatin microspheres versus gelatin sponge particles for leiomyoma. Cardiovasc Intervent Radiol. 2017;40:1687–93.
Chiu CY, Wong WK, Mak HL, Chan CS, Kwok CH, Chan CH, Chan MK. Uterine artery embolisation for treatment of fibroids: experience in Chinese women. Singap Med J. 2001;42:148–54.
Kim HS, Czuczman GJ, Nicholson WK, Pham LD, Richman JM. Pain levels within 24 hours after UFE: a comparison of morphine and fentanyl patient-controlled analgesia. Cardiovasc Intervent Radiol. 2008;31:1100–7.
McCullough M, et al. Polyvinyl alcohol particles and tris-acryl gelatin microspheres for uterine artery embolization for leiomyomas: results of a randomized comparative study. J Vasc Interv Radiol. 2012;15:793–800.
Rasuli P, et al. Outpatient uterine artery embolization for symptomatic fibroids: short- and long-term single institution-based outcomes. J Obstet Gynaecol Canada. 2013;35:156–63.
Barnard EP, et al. Periprocedural outcomes comparing fibroid embolization and focused ultrasound: a randomized controlled trial and comprehensive cohort analysis. Am J Obs Gynecol. 2017;216:87–97.
Tran C, et al. Tolerance, hospital stay, and recovery after uterine artery embolization for fibroids: the Ontario uterine fibroid embolization trial. J Vasc Interv Radiol. 2012;14:1243–50.
Cunningham E, Barreda L, Ngo M, Terasaki K, Munro MG. Uterine artery embolization versus occlusion for uterine leiomyomas: a pilot randomized clinical trial. J Minim Invasive Gynecol. 2008;15:301–7.
Jensen LL, et al. No morphine sparing effect of ketamine added to morphine for patient-controlled intravenous analgesia after uterine artery embolization. Acta Anaesthesiol Scand. 2008;52:479–86.
Pisco JM, Bilhim T, Duarte M, Santos D. Management of uterine artery embolization for fibroids as an outpatient procedure. J Vasc Interv Radiol. 2009;20:730–5.
Manninen H, Hippeläinen M, Ruuskanen A, Sipola P, Wüstefeld M. Pain after uterine fibroid embolisation is associated with the severity of myometrial ischaemia on magnetic resonance imaging. Eur Radiol. 2009;19:2977–85.
Konstantatos AH, et al. A randomized, double-blind, placebo-controlled study of preemptive oral oxycodone with morphine patient-controlled anesthesia for postoperative pain management in patients undergoing uterine artery embolization for symptomatic uterine fibroids. Cardiovasc Intervent Radiol. 2014;37:1191–7.
Roth AR, et al. Pain after uterine artery embolization for leiomyomata: can its severity be predicted and does severity predict outcome? J Vasc Interv Radiol. 2007;11:1047–52.
Yoon J, et al. Superior hypogastric nerve block as post-uterine artery embolization analgesia: a randomized and double-blind clinical trial. Radiology. 2018;289:248–54.
Pisco JM, Tsuchiya M, Bilhim T, Duarte M, Santos D, Oliveira AG. Uterine artery embolization under electroacupuncture for uterine leiomyomas. J Vasc Interv Radiol. 2009;20(7):863–70.
Freire GMG, et al. Controlled-release oxycodone improves pain management after uterine artery embolisation for symptomatic fibroids. Clin Radiol. 2017. https://doi.org/10.1016/j.crad.2016.12.010.
Rasuli P, et al. Superior hypogastric nerve block for pain control in outpatient uterine artery embolization. J Vasc Interv Radiol. 2004;15:1423–9.
Hehenkamp WJK, Volkers NA, Birnie E, Reekers JA, Ankum WM. Pain and return to daily activities after uterine artery embolization and hysterectomy in the treatment of symptomatic uterine fibroids: results from the randomized EMMY trial. Cardiovasc Intervent Radiol. 2006;29:179–87.
Keyoung JA, et al. Intraarterial lidocaine for pain control after uterine artery embolization for leiomyomata. J Vasc Interv Radiol. 2001;12:1065–9.
Noel-Lamy M, et al. Intraarterial lidocaine for pain control in uterine artery embolization: a prospective, randomized study. J Vasc Interv Radiol. 2017;28:16–22.
Bilhim T, Pisco JM, Duarte M, Oliveira AG. Polyvinyl alcohol particle size for uterine artery embolization: a prospective randomized study of initial use of 350–500 μm particles versus initial use of 500–700 μm particles. J Vasc Interv Radiol. 2011;22:21–7.
Kim SY, et al. Comparison of the efficacy of dexmedetomidine plus fentanyl patient-controlled analgesia with fentanyl patient-controlled analgesia for pain control in uterine artery embolization for symptomatic fibroid tumors or adenomyosis: a prospective, randomized st. J Vasc Interv Radiol. 2013;24:779–86.
Kim SY, et al. The effects of single-dose dexamethasone on inflammatory response and pain after uterine artery embolisation for symptomatic fibroids or adenomyosis: a randomised controlled study. BJOG An Int J Obstet Gynaecol. 2016;123:580–7.
Plancarte R, de Leon-Casasola OA, El-Helaly M, Allende S, Lema MJ. Neurolytic superior hypogastric plexus block for chronic pelvic pain associated with cancer. Reg Anesth. 1997;22(6):562–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare they have no conflict of interest.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed Consent
For this type of study, informed consent is not required.
Consent for Publication
For this type of study, consent for publication is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Saibudeen, A., Makris, G.C., Elzein, A. et al. Pain Management Protocols During Uterine Fibroid Embolisation: A Systematic Review of the Evidence. Cardiovasc Intervent Radiol 42, 1663–1677 (2019). https://doi.org/10.1007/s00270-019-02327-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-019-02327-1