
Abstract
Introduction
The UK Registry of Prostate Artery Embolization (UK-ROPE) was a prospective, multicentre study comparing PAE against surgical therapies for symptomatic benign prostatic hyperplasia (BPH). A wealth of data was collected supplementary to the main study outcomes which provide a snapshot of UK PAE practice. We aimed to interpret these data in the hope of providing insight into factors which affect clinical outcome and radiation dose.
Methods
216 patients (mean age 66, mean IPSS 21.3) undergoing PAE at 20 British centres from July 2014 to January 2016 were prospectively followed up to 12 months with retrospective analysis of the data. Technical outcome was evaluated based on procedural and fluoroscopy times, skin dose and dose area product (DAP). Clinical outcome was evaluated through collection of Qmax, IPSS reduction and prostate volume reduction. Multiple analysis of variance (MANOVA) was used to assess the significance of various patients and procedural factors on clinical outcome and patient dose.
Results
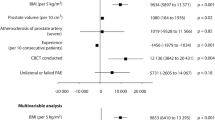
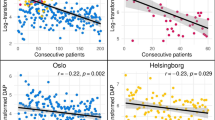
Significant predictors of technical outcome which affected patient skin dose included severity of CTA-detected atheroma (p < 0.001), the practitioner (p < 0.001) and use of protective coil embolization (p = 0.019). Predictors of clinical outcome included initial prostate size (dichotomized into groups > 80 ml and = <80 ml, d = 1, p = 0.0138), embolic agent (spherical particles < 300 nm performed best, p = 0.01) and number of arteries embolized (IPSS reduction of 32.9% in unilateral PAE versus 54.4% for bilateral PAE, p = 0.026).
Conclusion
We have identified several important factors which are associated with improved clinical outcome and increased patient dose which we hope will facilitate optimal patient selection and encourage improved embolization technique.






Similar content being viewed by others
References
Wang X-Y, Zong H-T, Zhang Y. Efficacy and safety of prostate artery embolization on lower urinary tract symptoms related to benign prostatic hyperplasia: a systematic review and meta-analysis. Clin Interv Aging. 2016;11(11):1609–22.
Bhatia S. Meta-analysis of prostatic artery embolization for benign prostatic hyperplasia-review of 12-month outcomes data. J Vasc Interv Radiol. 2017;28(5):772.
Pyo J-S, Cho WJ. Systematic review and meta-analysis of prostatic artery embolisation for lower urinary tract symptoms related to benign prostatic hyperplasia. Clin Radiol. 2017;72(1):16–22.
Shim SR, Kanhai KJK, Ko YM, Kim JH. Efficacy and safety of prostatic arterial embolization: systematic review with meta-analysis and meta-regression. J Urol. 2017;197(2):465–79.
BSIR UK-ROPE registry information [Internet]. [cited 2018 Jun 18]. Available from: https://www.bsir.org/registries/uk-rope-registry-of-prostate-embolisation/.
Ray AF, Powell J, Speakman MJ, Longford NT, DasGupta R, Bryant T, et al. Efficacy and safety of prostate artery embolization for benign prostatic hyperplasia: an observational study and propensity-matched comparison with transurethral resection of the prostate (the UK-ROPE study). BJU Int [Internet]. 2018 Apr 12; Available from: http://dx.doi.org/10.1111/bju.14249.
NICE Interventional procedures guidance 611 [Internet]. NICE. Available from: nice.org.uk/guidance/ipg611.
Wang M, Guo L, Duan F, Yuan K, Zhang G, Li K, et al. Prostatic arterial embolization for the treatment of lower urinary tract symptoms caused by benign prostatic hyperplasia: a comparative study of medium- and large-volume prostates. BJU Int. 2016;117(1):155–64.
Maclean D, Harris M, Drake T, Maher B, Modi S, Dyer J, et al. Factors Predicting a Good Symptomatic Outcome After Prostate Artery Embolisation (PAE). Cardiovasc Intervent Radiol [Internet]. 2018 Feb 26; Available from: http://dx.doi.org/10.1007/s00270-018-1912-5.
Wang MQ, Guo LP, Zhang GD, Yuan K, Li K, Duan F, et al. Prostatic arterial embolization for the treatment of lower urinary tract symptoms due to large (> 80 mL) benign prostatic hyperplasia: results of midterm follow-up from Chinese population. BMC Urol [Internet]. 2015;15(1). Available from: http://dx.doi.org/10.1186/s12894-015-0026-5.
Pisco JM, Rio Tinto H, Campos Pinheiro L, Bilhim T, Duarte M, Fernandes L, et al. Embolisation of prostatic arteries as treatment of moderate to severe lower urinary symptoms (LUTS) secondary to benign hyperplasia: results of short- and mid-term follow-up. Eur Radiol. 2013;23(9):2561–72.
Bagla S, Smirniotopoulos JB, Orlando JC, van Breda A, Vadlamudi V. Comparative analysis of prostate volume as a predictor of outcome in prostate artery embolization. J Vasc Interv Radiol. 2015;26(12):1832–8.
Kurbatov D, Russo GI, Lepetukhin A, Dubsky S, Sitkin I, Morgia G, et al. Prostatic artery embolization for prostate volume greater than 80 cm3: results from a single-center prospective study. Urology. 2014;84(2):400–4.
Little MW, Boardman P, Macdonald AC, Taylor N, Macpherson R, Crew J, et al. Adenomatous-dominant benign prostatic hyperplasia (AdBPH) as a predictor for clinical success following prostate artery embolization: an age-matched case-control study. Cardiovasc Intervent Radiol. 2017;40(5):682–9.
de Assis AM, Maciel MS, Moreira AM, de Paula Rodrigues VC, Antunes AA, Srougi M, et al. Prostate zonal volumetry as a predictor of clinical outcomes for prostate artery embolization. Cardiovasc Intervent Radiol. 2017;40(2):245–51.
Bilhim T, Pisco J, Pereira JA, Costa NV, Fernandes L, Campos Pinheiro L, et al. Predictors of clinical outcome after prostate artery embolization with spherical and nonspherical polyvinyl alcohol particles in patients with benign prostatic hyperplasia. Radiology. 2016;281(1):289–300.
Gonçalves OM, Carnevale FC, Moreira AM, Antunes AA, Rodrigues VC, Srougi M. Comparative study using 100-300 versus 300-500 μm microspheres for symptomatic patients due to enlarged-BPH prostates. Cardiovasc Intervent Radiol. 2016;39(10):1372–8.
Bilhim T, Pisco J, Campos Pinheiro L, Rio Tinto H, Fernandes L, Pereira JA, et al. Does polyvinyl alcohol particle size change the outcome of prostatic arterial embolization for benign prostatic hyperplasia? results from a single-center randomized prospective study. J Vasc Interv Radiol. 2013;24(11):1595.
de Assis AM, Moreira AM, de Paula Rodrigues VC, Yoshinaga EM, Antunes AA, Harward SH, et al. Prostatic artery embolization for treatment of benign prostatic hyperplasia in patients with prostates > 90 g: a prospective single-center study. J Vasc Interv Radiol. 2015;26(1):87–93.
Amouyal G, Thiounn N, Pellerin O, Yen-Ting L, Del Giudice C, Dean C, et al. Clinical results after prostatic artery embolization using the perfected technique: a single-center study. Cardiovasc Intervent Radiol. 2016;39(3):367–75.
Kisilevzky N, Faintuch S. MRI assessment of prostatic ischaemia: best predictor of clinical success after prostatic artery embolisation for benign prostatic hyperplasia. Clin Radiol. 2016;71(9):876–82.
Little MW, Macdonald AC, Boardman P, Bratby MJ, Anthony S, Hadi M, et al. Effects of sublingual glyceryl trinitrate administration on the quality of preprocedure CT angiography performed to plan prostate artery embolization. J Vasc Interv Radiol. 2018;29(2):225–8.
Bilhim T, Pisco JM, Rio Tinto H, Fernandes L, Pinheiro LC, Furtado A, et al. Prostatic arterial supply: anatomic and imaging findings relevant for selective arterial embolization. J Vasc Interv Radiol. 2012;23(11):1403–15.
Maclean D, Maher B, Harris M, Dyer J, Modi S, Hacking N, et al. Planning prostate artery embolisation: is it essential to perform a pre-procedural CTA? Cardiovasc Intervent Radiol. 2018;41(4):628–32.
Bilhim T, Pisco JM, Duarte M, Oliveira AG. Polyvinyl alcohol particle size for uterine artery embolization: a prospective randomized study of initial use of 350-500 μm particles versus initial use of 500-700 μm particles. J Vasc Interv Radiol. 2011;22(1):21–7.
Funding
The UK-ROPE study was funded through multiple streams. The involvement of an independent academic evaluation centre ‘Cedar’ was funded through the National Institute for Health and Care Excellence (NICE). Procedure costs were covered either through local commissioning streams or through a grant from Cook Medical (Europe), where this was not possible.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Nigel Hacking was in receipt of a research grant to run the UK-ROPE study from Cook Medical, has received honoraria from Boston Scientific and Celonova as a speaker and has been on Advisory boards for BTG. Tim Bryant has proctored for Boston Scientific and Terumo and has received speaker honorariums from Boston Scientific. Sachin Modi has received a speaker honorarium from Boston Scientific. The other authors declare no conflict of interest.
Ethical Approval
All procedures performed were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Patient Consent
Informed consent was obtained from all individual participants included in the study. Consent for publication was obtained for every individual person’s data included in the study.
Rights and permissions
About this article

Cite this article
Hacking, N., Vigneswaran, G., Maclean, D. et al. Technical and Imaging Outcomes from the UK Registry of Prostate Artery Embolization (UK-ROPE) Study: Focusing on Predictors of Clinical Success. Cardiovasc Intervent Radiol 42, 666–676 (2019). https://doi.org/10.1007/s00270-018-02156-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-018-02156-8