
Abstract
Purpose
To prospectively assess discontinuation of indwelling bladder catheterization (IBC) and relief of lower urinary tract symptoms (LUTS) due to benign prostatic hyperplasia (BPH) following prostate artery embolization (PAE) in poor surgical candidates.
Methods
Patients ineligible for surgical intervention were offered PAE after at least 1 month of IBC for management of urinary retention secondary to BPH; exclusion criteria for PAE included eligibility for surgery, active bladder cancer or known prostate cancer. Embolization technical and clinical success were defined as bilateral prostate embolization and removal of IBC, respectively. Patients were followed for at least 6 months and evaluated for International Prostate Symptom Score, quality of life, prostate size and uroflowmetric parameters.
Results
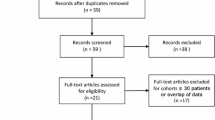
A total of 43 patients were enrolled; bilateral embolization was performed in 33 (76.7%), unilateral embolization was performed in 8 (18.6%), and two patients could not be embolized due to tortuous and atherosclerotic pelvic vasculature (4.7%). Among the patients who were embolized, mean prostate size decreased from 75.6 ± 33.2 to 63.0 ± 23.2 g (sign rank p = 0.0001, mean reduction of 19.6 ± 17.3%), and IBC removal was achieved in 33 patients (80.5%). Clavien II complications were reported in nine patients (21.9%) and included urinary tract infection (three patients, 7.3%) and recurrent acute urinary retention (six patients, 14.6%). Nine patients (22.0%) experienced post-embolization syndrome.
Conclusions
PAE is a safe and feasible for the relief of LUTS and IBC in highly comorbid patients without surgical treatment options.


Similar content being viewed by others


References
Irwin DE, Kopp ZS, Agatep B, Milsom I, Abrams P. Worldwide prevalence estimates of lower urinary tract symptoms, overactive bladder, urinary incontinence and bladder outlet obstruction. BJU Int. 2011;108:1132–8.
Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2163–96.
European Association of Urology. Guidelines on the management of non-neurogenic male lower urinary tract symptoms (LUTS), incl. benign prostatic obstruction (BPO) (2014). http://uroweb.org/wp-content/uploads/EAU-Guidelines-Non-Neurogenic-Male-LUTS-Guidelines-2015-v2.pdf. Accessed 4 Mar 2015.
American Urological Association. Guideline: management of benign prostatic hyperplasia (rev. 2010). https://www.auanet.org/common/pdf/education/clinical-guidance/Benign-Prostatic-Hyperplasia.pdf. Accessed 10 May 2015.
Carnevale FC, Antunes AA, da Motta Leal Filho JM, Cerri LMO, Baroni RH, Marcelino ASZ, et al. Prostatic artery embolization as a primary treatment for benign prostatic hyperplasia: preliminary results in two patients. Cardiovasc Interv Radiol. 2010;. doi:10.1007/s00270-009-9727-z.
Pisco J, Pinheiro LC, Bilhim T, Duarte M, Rio Tinto H, Fernandes L, et al. Prostatic arterial embolization for benign prostatic hyperplasia: short- and intermediate-term results. Radiology. 2013;. doi:10.1148/radiol/12111601.
Kurbatov D, Russo GI, Lepetukhin A, Dubsky S, Sitkin I, Morgia G, et al. Prostatic artery embolization for prostate volume greater than 80 cm3: results from a single-center prospective study. Urology. 2014;84:400–4.
Antunes AA, Carnevale FC, da Motta Leal Filho JM, Yoshinaga EM, Cerri LMO, Baroni RH, et al. Clinical, laboratorial, and urodynamic findings of prostatic artery embolization for the treatment of urinary retention related to benign prostatic hyperplasia: a prospective, single-center pilot study. Cardiovasc Interv Radiol. 2013;. doi:10.1007/s00270-013-0611-5.
de Assis AM, Moreira AM, de Paula Rodrigues VC, Yoshinaga EM, Antunes AA, Harward SH, et al. Prostatic artery embolization for treatment of benign prostatic hyperplasia in patients with prostates >90 g: a prospective, single-center study. J Vasc Interv Radiol. 2015;26:87–93.
Grosso M, Balderi A, Arnò M, Sortino D, Antonietti A, Pedrazzini R, et al. Prostatic artery embolization in benign prostatic hyperplasia: preliminary results in 13 patients. Radiol Med. 2014;. doi:10.1007/s11547-014-0447-3.
Bhatia S, Kava B, Pereira K, Kably I, Harward S, Narayanan G. Prostate artery embolization for giant prostatic hyperplasia. J Vasc Interv Radiol. 2015;26:1583–5.
Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47:1245–51.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–13.
European Association of Urology. Guidelines on reporting and grading of complications after urologic surgical procedures. http://uroweb.org/wp-content/uploads/30-Reporting-complications_LR.pdf. Accessed 1 Dec 2015.
Carnevale FC, Moreira AM, Antunes AA. The “PErFecTED technique”: proximal embolization first, then embolize distal for benign prostatic hyperplasia. Cardiovasc Interv Radiol. 2014;. doi:10.1007/s00270-014-0908-z.
Fabian KM. The intra-prostatic “partial catheter” (urological spiral). Urologe A. 1980;19:236–8.
Armitage JN, Cathcart PJ, Rashidian A, de Nigris E, Emberton M, van der Meulen JHP. Epithelializing stent for benign prostatic hyperplasia: a systematic review of the literature. J Urol. 2007;177:1619–24.
Silva J, Silva C, Saraiva L, Silva A, Pinto R, Dinis P, et al. Intraprostatic Botulium toxin type A injection in patients unfit for surgery presenting with refractory urinary retention and benign prostatic enlargement: effect on prostate volume and micturition resumption. Euro Urol. 2008;53:153–9.
Marberger M, Chartier-Kastler E, Egerdie B, Lee KS, Grosse J, Bugarin D, et al. A randomized double-blind placebo-controlled phase 2 dose-ranging study of onabotulinumtoxinA in men with benign prostatic hyperplasia. Eur Urol. 2013;63:496–503.
Magno C, Mucciardi G, Gali A, Anastasi G, Inferrera A, Morgia G. Transurethral ethanol ablation of the prostate (TEAP): an effective minimally invasive treatment alternative to traditional surgery for symptomatic benign prostatic hyperplasia (BPH) in high-risk comorbidity patients. Int Urol Nephrol. 2008;40:941–6.
Grise P, Plante M, Palmer J, Martinez-Sagarra J, Hernandez C, Schettini M, et al. Evaluation of the transurethral ethanol ablation of the prostate (TEAP) for symptomatic benign prostatic hyperplasia (BPH): a European multi-center evaluation. Eur Urol. 2004;46:496–501.
Ikari O, Leitão VA, D’Ancona CAL, Matheus WE, Netto NR. Intravesical calculus secondary to ethanol gel injection into the prostate. Urol. 2005;65:1002.
Wang MQ, Wang Y, Yan JY, Yuan K, Zhang GD, Duan F, Li K. Prostatic artery embolization for the treatment of symptomatic benign prostatic hyperplasia in men ≥75 years: a prospective single-center study. World J Urol. 2016;34:1275–1283.
Carnevale FC, Antunes AA. Prostatic artery embolization for enlarged prostates due to benign prostatic hyperplasia: how I do it. Cardiovasc Interv Radiol. 2013;. doi:10.1007/s00270-013-0680-5.
Schäfer W, Abrams P, Liao L, Mattiasson A, Pesce F, Spangberg A, et al. Good urodynamic practices: uroflowmetry, filling cystometry, and pressure-flow studies. Neurourol Urodyn. 2002;21:261–74.
Moreira AM, Marques CFS, Antunes AA, Nahas CSR, Nahas SC, de Gregorio Ariza MA, et al. Transient ischemic rectitis as a potential complication after prostatic artery embolization: case report and review of the literature. Cardiovasc Interv Radiol. 2013;. doi:10.1007/s00270-013-0739-3.
Pisco JM, Pinheiro LC, Bilhim T, Duarte M, Mendes JR, Oliveira AG. Prostatic arterial embolization to treat benign prostatic hyperplasia. J Vasc Interv Radiol. 2011;22:11–9.
Bilhim T, Pisco JM, Furtado A, Casal D, Pais D, Pinheiro LC, et al. Prostatic arterial supply: demonstration by multirow detector angio CT and catheter angiography. Eur Radiol. 2011;21:1119–26.
Bagla S, Rholl KS, Sterling KM, van Breda A, Papadouris D, Cooper JM, et al. Utility of cone-beam CT imaging in prostatic artery embolization. J Vasc Interv Radiol. 2013;24:1603–7.
Laborda A, de Assis AM, Ioakeim I, Sánchez-Ballestín M, Carnevale FC, de Gregorio MA. Radiodermitis after prostatic artery embolization: case report and review of the literature. Cardiovasc Interv Radiol. 2015;. doi:10.1007/s00270-015-1083-6.
Lin YT, Amouyal G, Thiounn N, Pellerin O, Pereira H, Del Giudice C, et al. Intra-vesical prostatic protrusion (IPP) can be reduced by prostatic artery embolization. Cardiovasc Interv Radiol. 2015;. doi:10.1007/s00270-015-1235-8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
SHH and FCC are consultants for Merit Medical Systems, Inc.
Rights and permissions
About this article

Cite this article
Rampoldi, A., Barbosa, F., Secco, S. et al. Prostatic Artery Embolization as an Alternative to Indwelling Bladder Catheterization to Manage Benign Prostatic Hyperplasia in Poor Surgical Candidates. Cardiovasc Intervent Radiol 40, 530–536 (2017). https://doi.org/10.1007/s00270-017-1582-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-017-1582-8