
Abstract
Introduction
The AAST liver injury grade has a validated association with mortality and need for operation. AAST liver injury grade is the same regardless of the mechanism of trauma.
Methods
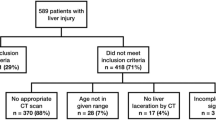
A 5-year retrospective review of all liver injuries at an urban, level-one trauma center was performed.
Results
Totally, 315 patients were included (29% blunt, 71% penetrating). In blunt trauma, AAST grade was associated with need for laparotomy (0%, 7%, 5%, 33%, 29%, Grade 1–5, p = 0.01), angiography (0%, 7%, 25%, 40%, 57%, p < 0.001), embolization (0%, 7%, 15%, 33%, 43%, p = 0.01), and percutaneous drainage procedures (13% use in Grade 4, otherwise 0%, p = 0.04), but not ERCP (0% for all grades). In penetrating trauma, AAST grade was associated with need for angiography (7%, 4%, 15%, 24%, 30%, p < 0.01) and percutaneous drainage (7%, 2%, 14%, 18%, 26%, p = 0.03) and had a marginal association with embolization (0%, 4%, 11%, 13%, 22%, p = 0.06). Laparotomy, ERCP, sphincterotomy, and stenting rates increased with AAST grade, but this was not statistically significant.
Conclusion
AAST grade is associated with the need for surgical hemostasis, angioembolization, and percutaneous drainage in both penetrating and blunt trauma. Operative, endoscopic, and percutaneous procedures are utilized more in penetrating trauma. Angioembolization was used more in blunt trauma. Mechanism should be considered when using AAST grade to guide management of liver injuries.





Similar content being viewed by others


References
Moore EE, Shackford SR, Pachter HL et al (1989) Organ injury scaling: spleen, liver, and kidney. J Trauma 29(12):1664–1666
Petrowsky H, Raeder S, Zuercher L et al (2012) A quarter century experience in liver trauma: a plea for early computed tomography and conservative management for all hemodynamically stable patients. World J Surg 36:247–254. https://doi.org/10.1007/s00268-011-1384-0
Asensio JA, Demetriades D, Chahwan S et al (2000) Approach to the management of complex hepatic injuries. J Trauma 48(1):67–70
Asensio JA, Petron P, García-Núñez L et al (2007) Multidisciplinary approach for the management of complex hepatic injuries AAST-OIS grades IV–V: a prospective study. Scand J Surg 96:214–220
Asensio JA, Roldán G, Petrone P et al (2003) Operative management and outcomes in 103 AAST-OIS grades IV and V complex hepatic injuries: trauma surgeons still need to operate, but angioembolization helps. J Trauma 54:647–654
MacKenzie S, Kortbeek JB, Mulloy R et al (2004) Recent experiences with a multidisciplinary approach to complex hepatic trauma. Injury Int J Care Injured 35:869–877
Matsushima K, Hogen R, Piccinini A et al (2020) Adjunctive use of hepatic angioembolization following hemorrhage control laparotomy. J Trauma Acute Care Surg. 88:636–643
Harrell DJ, Vitale GC, Larson GM (1998) Selective role for endoscopic retrograde cholangiopancreatography in abdominal trauma. Surg Endosc 12:400–404
Scollay JM, Beard D, Smith R et al (2005) Eleven years of liver trauma: the scottish experience. World J Surg 29:744–749. https://doi.org/10.1007/s00268-005-7752-x
Tinkoff G, Esposito TJ, Reed J et al (2008) American Association for the Surgery of Trauma Organ Injury Scale I: spleen, liver, and kidney, validation based on the National Trauma Data Bank. J Am Coll Surg 207:646–655
Kozar RA, Moore JB, Niles SE et al (2005) Complication of nonoperative management of high-grade blunt hepatic injuries. J Trauma 59:1066–1071
Kozar RA, Moore FA, Cothren CC et al (2006) Risk factors for hepatic morbidity following nonoperative management. Arch Surg 141:451–459
Dabbs DN, Stein DM, Scalea TM (2009) Major hepatic necrosis: a common complication after angioembolization for treatment of high-grade liver injuries. J Trauma 66:621–629
Koch M, Garden OJ, Padbury R et al (2011) Bile leakage after hepatobiliary and pancreatic surgery: a definition and grading of severity by the International Study Group of Liver Surgery. Surgery 149:680–688
Kozar RA, Moore FA, Moore EE et al (2009) Western trauma association critical decisions in trauma: nonoperative management of adult blunt hepatic trauma. J Trauma 67(6):1144–1149
Stassen NA, Bhullar I, Cheng JD et al (2012) Nonoperative management of blunt hepatic injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg 73(5):S288-293
Coccolini F, Coimbra R, Ordonez C et al (2020) Liver trauma: WSES 2020 guidelines. World J Emerg Surg 15(24):1–15
Slotta JE, Justinger C, Kollmar O et al (2014) Liver injury following blunt abdominal trauma: a new mechanism-driven classification. Surg Toay 44:241–246
Jin W, Deng L, Heping LV et al (2013) Mechanisms of blunt liver trauma patterns: an analysis of 53 cases. Exp Ther Med 5:395–398
Sardiwalla I, Govender M, Matsevych O et al (2016) Indirect ballistic injury to the liver: case report and review of the literature. Int J Surg Open 5:23–26
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no financial support and no pharmaceutical and industry support.
Ethical approval
This study was approved by the IRB of Cook County Health as a retrospective review with an exemption for consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Brigode, W., Adra, A., Capron, G. et al. The American Association for the Surgery of Trauma (AAST) Liver Injury Grade Does Not Equally Predict Interventions in Blunt and Penetrating Trauma. World J Surg 46, 2123–2131 (2022). https://doi.org/10.1007/s00268-022-06595-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-022-06595-w