
Abstract
Background
Risk stratification has become a key part of the care processes for patients having emergency bowel surgery. This study aimed to determine if operative approach influences risk-model performance, and risk-adjusted mortality rates in the United Kingdom.
Methods
A prospectively planned analysis was conducted using National Emergency Laparotomy Audit (NELA) data from December 2013 to November 2018. The risk-models investigated were P-POSSUM and the NELA Score, with model performance assessed in terms of discrimination and calibration. Risk-adjusted mortality was assessed using Standardised Mortality Ratios (SMR). Analysis was performed for the total cohort, and cases performed open, laparoscopically and converted to open. Sub-analysis was performed for cases with ≤ 20% predicted mortality.
Results
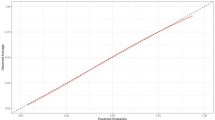
Data were available for 116 396 patients with P-POSSUM predicted mortality, and 46 935 patients with the NELA score. Both models displayed excellent discrimination with little variation between operative approaches (c-statistic: P-POSSUM 0.801–0.836; NELA Score 0.811–0.862). The NELA score was well calibrated across all deciles of risk, but P-POSSUM over-predicted risk beyond 20% mortality. Calibration plots for operative approach demonstrated that both models increasingly over-predicted mortality for laparoscopy, relative to open and converted to open surgery. SMRs calculated using both models consistently demonstrated that risk-adjusted mortality with laparoscopy was a third lower than open surgery.
Conclusion
Risk-adjusted mortality for emergency bowel surgery is lower for laparoscopy than open surgery, with P-POSSUM and NELA score both over-predicting mortality for laparoscopy. Operative approach should be considered in the development of future risk-models that rely on operative data.



Similar content being viewed by others


References
The NELA Project Team (2020) Sixth Patient Report of the National Emergency Laparotomy Audit. 1–51 https://www.nela.org.uk/reports
Oliver CM et al (2018) Organisational factors and mortality after an emergency laparotomy: multilevel analysis of 39 903 national emergency laparotomy audit patients. BJA 121:1346–1356
Aggarwal G et al (2019) Evaluation of the collaborative use of an evidence-based care bundle in emergency laparotomy. JAMA Surg 154:e190145–e190210
Prytherch DR et al (1998) POSSUM and Portsmouth POSSUM for predicting mortality. Br J Surg 85:1217–1220
Eugene N et al (2018) Development and internal validation of a novel risk adjustment model for adult patients undergoing emergency laparotomy surgery: the national emergency laparotomy audit risk model. Br J Anaesth 121:739–748
Moonesinghe SR, Mythen MG, Das P, Rowan KM, Grocott MPW (2013) Risk stratification tools for predicting morbidity and mortality in adult patients undergoing major surgery. Anesthesiology 119:959–981
Oliver CM, Walker E, Giannaris S, Grocott MPW, Moonesinghe SR (2015) Risk assessment tools validated for patients undergoing emergency laparotomy: a systematic review. BJA 115:849–860
Boyd-Carson H et al (2020) The association of pre-operative anaemia with morbidity and mortality after emergency laparotomy. Anaesthesia 75:904–912
Jarman B et al (1999) Explaining differences in English hospital death rates using routinely collected data. BMJ 318:1515–1520
Iezzoni LI (1997) The risks of risk adjustment. JAMA 278:1600–1607
Guillou PJ et al (2005) Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. Lancet (London, England) 365:1718–1726
Jayne DG et al (2010) Five-year follow-up of the Medical Research Council CLASICC trial of laparoscopically assisted versus open surgery for colorectal cancer. Br J Surg 97:1638–1645
Biere SSAY et al (2012) Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: a multicentre, open-label, randomised controlled trial. Lancet (London, England) 379:1887–1892
van der Pas MH et al (2013) Laparoscopic versus open surgery for rectal cancer (COLOR II): short-term outcomes of a randomised, phase 3 trial. Lancet Oncol 14:210–218
Bonjer HJ et al (2015) A randomized trial of laparoscopic versus open surgery for rectal cancer. N Engl J Med 372:1324–1332
Mariette C et al (2019) Hybrid minimally invasive Esophagectomy for Esophageal cancer. N Engl J Med 380:152–162
Calster BV et al (2019) Calibration: the Achilles heel of predictive analytics. BMC Med 17:230–237
DeLong ER, DeLong DM, Clarke-Pearson DL (1988) Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 44:837–845
von Elm E et al (2008) The strengthening the reporting of observational studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol 61:344–349
The NELA Project Team (2017) Third patient report of the national emergency laparotomy audit (NELA). 1–190 https://www.nela.org.uk/downloads/The%20Third%20Patient%20Report%20of%20the%20National%20Emergency%20Laparotomy%20Audit%202017%20-%20Full%20Patient%20Report.pdf
Mohammed MA et al (2009) Evidence of methodological bias in hospital standardised mortality ratios: retrospective database study of English hospitals. BMJ 338:b780–b788
Heywood N et al (2021) The laparoscopy in emergency general surgery (LEGS) study: a questionnaire survey of UK practice. Ann Royal Coll Surg Engl 103:120–129
The NELA Project Team (2015) The First Patient Report of the National Emergency Laparotomy Audit. 1–151 https://www.nela.org.uk/All-Patient-Reports.
Badrick E, et al. (2020) Laparoscopy in emergency general surgery (The LEGS Study): NELA database analysis. B J Surg
Bilimoria KY, Liu Y, Paruch JL, Zhou L, Kmiecik TE, Ko CY, Cohen ME (2013) Development and evaluation of the universal ACS NSQIP surgical risk calculator: a decision aid and informed consent tool for patients and surgeons. J Am College Surg 217(5):833-842.e3
Liu Y, Cohen ME, Hall BL, Ko CY, Bilimoria KY (2016) Evaluation and enhancement of calibration in the American college of surgeons NSQIP surgical risk calculator. J Am Coll Surg 223:231–239
Bertsimas D, Dunn J, Velmahos GC, Kaafarani HMA (2018) Surgical risk is not linear: derivation and validation of a novel, user-friendly, and machine-learning-based predictive optimal trees in emergency surgery risk (POTTER) calculator. Ann Surg 268:574–583
Pucher PH, Mackenzie H, Tucker V, Mercer SJ (2021) A national propensity score-matched analysis of emergency laparoscopic versus open abdominal surgery. B J Surg. https://doi.org/10.1093/bjs/znab048
Sallinen V et al (2019) Laparoscopic versus open adhesiolysis for adhesive small bowel obstruction (LASSO): an international, multicentre, randomised, open-label trial. Lancet Gastroenterol Hepatol 4:278–286
Harji DP et al (2020) Laparoscopic versus open colorectal surgery in the acute setting (LaCeS trial): a multicentre randomized feasibility trial. Br J Surg 107:1595–1604
Søreide K, Thorsen K, Søreide JA (2014) Strategies to improve the outcome of emergency surgery for perforated peptic ulcer. Br J Surg 101:e51-64
Moghadamyeghaneh Z, Talus H, Ballantyne G, Stamos MJ, Pigazzi A (2020) Short-term outcomes of laparoscopic approach to colonic obstruction for colon cancer. Surg Endosc. https://doi.org/10.1007/s00464-020-07743-w
Darbyshire AR, Kostakis I, Pucher PH, Toh S, Mercer SJ (2021) The impact of laparoscopy on emergency surgery for adhesional small bowel obstruction: prospective single centre cohort study. Annals Royal College Surg England. https://doi.org/10.1308/rcsann.2020.7079
Shibata J et al (2015) Surgical stress response after colorectal resection: a comparison of robotic, laparoscopic, and open surgery. Tech Coloproctol 19:275–280
Crippa J, Mari GM, Miranda A, Costanzi ATM, Maggioni D (2018) Surgical stress response and enhanced recovery after laparoscopic surgery - a systematic review. Chirurgia 113:455–510
Foss NB, Kehlet H (2020) Challenges in optimising recovery after emergency laparotomy. Anaesthesia 75:A4876–A4877
Martin P (2020) NELA risk adjustment model: recalibration of predictor coefficients. 1–6 https://data.nela.org.uk/getattachment/Support/NELA-Risk-Adjustment-Model/NELA-(2020)-Recalibrated-risk-model-coefficients.pdf.aspx?lang=en-GB
Funding
This project has not received any research funding.
Author information
Authors and Affiliations
Contributions
Project initiation: SM and AD. Planning of statistical analysis: AD, IK, DP and PP. Cleaning and analysis of data: AD, IK and SM. Interpretation of results: AD, IK, DP, PP and SM. Drafting of initial version of paper: AD and IK. Revision of paper: AD, IK, DP, PP and SM.
Corresponding author
Ethics declarations
Conflicts of interest
There are no conflicts of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Darbyshire, A.R., Kostakis, I., Pucher, P.H. et al. P-POSSUM and the NELA Score Overpredict Mortality for Laparoscopic Emergency Bowel Surgery: An Analysis of the NELA Database. World J Surg 46, 552–560 (2022). https://doi.org/10.1007/s00268-021-06404-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-021-06404-w