
Abstract
Background
Incisional hernia (IH) may occur in 20% of patients after laparotomy. The hernia sac volume may be of significance, with reintegration of visceral contents potentially leading to repair failure or abdominal compartment syndrome. The present study aimed to evaluate a two-step surgical strategy comprising right colectomy for hernia reduction with synchronous absorbable mesh repair followed by definitive non-absorbable mesh repair in recurrence.
Methods
Patients operated between 2012 and 2017 at two university centers were retrospectively included. Volumetric evaluation of the IH was performed by CT imaging.
Results
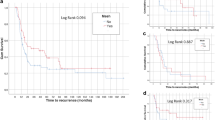
Eleven patients were included. The mean BMI was 43 kg/m2 (23–52 kg/m2). Progressive preoperative pneumoperitoneum was performed in 82% of patients, with complications in 22%. The mean volumetric ratio of the volume of the hernia to the volume of the abdominal cavity was 70% (48–100%). The first parietal repair was performed using an synthetic absorbable mesh (36%), a biologic mesh (27%), or a slowly absorbable mesh (36%). No patients died as a result of the procedure. Seven (64%) patients developed grade III–IV complications, including one case of an anastomotic fistula. Recurrence occurred in eight (73%) patients after the first repair. Of these, four (50%) patients were reoperated using a non-absorbable mesh, leading to solid repair in 75% of cases. After 27 ± 18 months of follow-up, the residual IH rate was 46%.
Conclusions
Right colectomy for volume reduction in IH with loss of domain potentially represents an appropriate salvage option, supporting bowel reintegration and temporary hernia repair with absorbable material.




Similar content being viewed by others

References
Fink C, Baumann P, Wente MN, Knebel P, Bruckner T, Ulrich A et al (2014) Incisional hernia rate 3 years after midline laparotomy: incisional hernia after midline laparotomy. Br J Surg 101(2):51–54
Bosanquet DC, Ansell J, Abdelrahman T, Cornish J, Harries R, Stimpson A et al (2015) Systematic review and meta-regression of factors affecting midline incisional hernia rates: analysis of 14 618 patients. PLoS ONE 10(9):e0138745
Blatnik JA, Brunt LM (2019) Controversies and techniques in the repair of abdominal wall hernias. J Gastrointest Surg 23(4):837–845
Slater NJ, Montgomery A, Berrevoet F, Carbonell AM, Chang A, Franklin M et al (2014) Criteria for definition of a complex abdominal wall hernia. Hernia 18(1):7–17
Chandeze M-M, Moszkowicz D, Bouillot J-L (2019) Large incisional hernias: the double layer technique with anterior component separation (with video). J Visc Surg 156(6):553–554
Ramirez OM, Ruas E, Dellon AL (1990) “Components separation” method for closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg 86(3):519–526
Tastaldi L, Blatnik JA, Krpata DM, Petro CC, Fafaj A, Alkhatib H et al (2019) Posterior component separation with transversus abdominis release (TAR) for repair of complex incisional hernias after orthotopic liver transplantation. Hernia J Hernias Abdom Wall Surg 23(2):363–373
Elstner KE, Read JW, Saunders J, Cosman PH, Rodriguez-Acevedo O, Jacombs ASW et al (2019) Selective muscle botulinum toxin A component paralysis in complex ventral hernia repair. Hernia. https://doi.org/10.1007/s10029-019-01939-3
Renard Y, Lardière-Deguelte S, de Mestier L, Appere F, Colosio A, Kianmanesh R et al (2016) Management of large incisional hernias with loss of domain: a prospective series of patients prepared by progressive preoperative pneumoperitoneum. Surgery 160(2):426–435
Sabbagh C, Dumont F, Fuks D, Yzet T, Verhaeghe P, Regimbeau J-M (2012) Progressive preoperative pneumoperitoneum preparation (the Goni Moreno protocol) prior to large incisional hernia surgery: volumetric, respiratory and clinical impacts. A prospective study. Hernia 16(1):33–40
Rogers WK, Garcia L (2018) Intraabdominal hypertension, abdominal compartment syndrome, and the open abdomen. Chest 153(1):238–250
Kirkpatrick AW, Roberts DJ, De Waele J, Jaeschke R, Malbrain MLNG, De Keulenaer B et al (2013) Intra-abdominal hypertension and the abdominal compartment syndrome: updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensive Care Med 39(7):1190–1206
Rosen MJ, Bauer JJ, Harmaty M, Carbonell AM, Cobb WS, Matthews B et al (2017) Multicenter, prospective, longitudinal study of the recurrence, surgical site infection, and quality of life after contaminated ventral hernia repair using biosynthetic absorbable mesh: the COBRA study. Ann Surg 265(1):205–211
Tanaka EY, Yoo JH, Rodrigues AJ, Utiyama EM, Birolini D, Rasslan S (2010) A computerized tomography scan method for calculating the hernia sac and abdominal cavity volume in complex large incisional hernia with loss of domain. Hernia 14(1):63–69
Sabbagh C, Dumont F, Robert B, Badaoui R, Verhaeghe P, Regimbeau J-M (2011) Peritoneal volume is predictive of tension-free fascia closure of large incisional hernias with loss of domain: a prospective study. Hernia 15(5):559–565
Angelici A, Perotti B, Dezzi C, Amatucci C, Mancuso G, Caronna R, Palumbo P (2016) Measurement of intra-abdominal pressure in large incisional hernia repair to prevent abdominal compartmental syndrome. G Chir 37(1):31–36
Poghosyan T, Veyrie N, Corigliano N, Helmy N, Servajean S, Bouillot J-L (2012) Retromuscular mesh repair of midline incisional hernia with polyester standard mesh: monocentric experience of 261 consecutive patients with a 5-year follow-up. World J Surg 36(4):782–790
Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD et al (2009) The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg 250(2):187–196
Bueno-Lledó J, Torregrosa A, Ballester N, Carreño O, Carbonell F, Pastor PG et al (2017) Preoperative progressive pneumoperitoneum and botulinum toxin type A in patients with large incisional hernia. Hernia 21(2):233–243
Bueno-Lledó J, Torregrosa A, Jiménez R, Pastor PG (2018) Preoperative combination of progressive pneumoperitoneum and botulinum toxin type A in patients with loss of domain hernia. Surg Endosc 32(8):3599–3608
Parker SG, Halligan S, Blackburn S, Plumb AAO, Archer L, Mallett S et al (2019) What exactly is meant by “loss of domain” for ventral hernia? systematic review of definitions. World J Surg 43(2):396–404
Martre P, Sarsam M, Tuech J-J, Coget J, Schwarz L, Khalil H (2019) New, simple and reliable volumetric calculation technique in incisional hernias with loss of domain. Hernia. https://doi.org/10.1007/s10029-019-01990-0
Soltanizadeh S, Helgstrand F, Jorgensen LN (2017) Botulinum toxin a as an adjunct to abdominal wall reconstruction for incisional hernia. Plast Reconstr Surg Glob Open 5(6):e1358
Berger RL, Li LT, Hicks SC, Davila JA, Kao LS, Liang MK (2013) Development and validation of a risk-stratification score for surgical site occurrence and surgical site infection after open ventral hernia repair. J Am Coll Surg 217(6):974–982
Moszkowicz D, Bouillot J-L (2018) Biological mesh: from concept to clinical reality. J Visc Surg 155(5):347–348
Holihan JL, Nguyen DH, Nguyen MT, Mo J, Kao LS, Liang MK (2016) Mesh location in open ventral hernia repair: a systematic review and network meta-analysis. World J Surg 40(1):89–99
Goodenough CJ, Ko TC, Kao LS, Nguyen MT, Holihan JL, Alawadi Z et al (2015) Development and validation of a risk stratification score for ventral incisional hernia after abdominal surgery: hernia expectation rates in intra-abdominal surgery (the HERNIA Project). J Am Coll Surg 220(4):405–413
Chandeze M-M, Moszkowicz D, Beauchet A, Vychnevskaia K, Peschaud F, Bouillot J-L (2019) Ventral hernia surgery in morbidly obese patients, immediate or after bariatric surgery preparation: results of a case-matched study. Surg Obes Relat Dis 15(1):83–88
Sjöström L (2013) Review of the key results from the Swedish Obese Subjects (SOS) trial—a prospective controlled intervention study of bariatric surgery. J Intern Med 273(3):219–234
Funding
There are no financial disclosures to declare.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest regarding the content of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Human and animal rights
I hereby undersign and certificate that this article does not contain any studies with animals performed by any of the authors.
Informed consent
Informed consent was obtained from all patients prior to their inclusion in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Benoit, O., Moszkowicz, D., Milot, L. et al. Right Colectomy with Absorbable Mesh Repair as a Salvage Solution for the Management of Giant Incisional Hernia with Loss of Domain: Results of a Bicentric Study. World J Surg 44, 1762–1770 (2020). https://doi.org/10.1007/s00268-020-05395-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-020-05395-4