
Abstract
Background
The French transplant governing system defined “Rescue” (the so-called “Hors Tour”) livers as those livers which were declined for the five top-listed patients. This study compares the outcomes following liver transplantation (LT) in patients who received a donor liver through a rescue allocation (RA) procedure or according to MELD score priority (standard allocation, SA) and evaluates the impact on the graft pool of a proactive policy to accept RA grafts.
Methods
Data from all consecutive patients who underwent LT with SA or RA grafts from 2011 to 2015 were compared in terms of short- and long-term outcomes.
Results
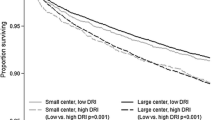
The 249 elective first LTs were performed with 64 (25.7%) RA and 185 (74.3%) SA grafts. RA grafts were obtained from older donors and were associated with a longer cold ischemia time. Recipients of RA livers were older and had lower MELD scores. The rates of delayed graft function, primary nonfunction, retransplantation, complications, and mortality were similar between the RA and SA groups. At 1 and 3 and 5 years, graft and patient survival rates were similar between the groups. These results were maintained after matching on recipient characteristics. Our proactive policy to accept RA grafts increased the liver pool for elective first transplantation by 25%.
Conclusions
RA livers can be safely transplanted into selected recipients and significantly expand the liver pool.




Similar content being viewed by others


References
Kim WR, Lake JR, Smith JM et al (2017) OPTN/SRTR 2015 annual data report: liver. Am J Transplant 17(Suppl 1):174–251
Eurotransplant International Foundation (2015) In: Branger P, Samuel U (eds) Annual report 2015. Eurotransplant Foundation, Leiden
Agence de la Biomedecine. Annual report 2014. https://www.agence-biomedecine.fr/annexes/bilan2014/donnees/organes/05-foie/pdf/hepatique.pdf
Lopez-Navidad A, Caballero F (2003) Extended criteria for organ acceptance. Strategies for achieving organ safety and for increasing organ pool. Clin Transplant 17(4):308–324
Durand F, Antoine C, Soubrane O (2019) Liver transplantation in France. Liver Transplant 25(5):763–770
Francoz C, Belghiti J, Castaing D et al (2011) Model for end-stage liver disease exceptions in the context of the French model for end-stage liver disease score-based liver allocation system. Liver Transplant 17(10):1137–1151
Jasseron C, Francoz C, Antoine C et al (2019) Impact of the new MELD-based allocation system on waiting list and post-transplant survival—a cohort analysis using the French national CRISTAL database. Transpl Int 32(10):1061–1073
Pezzati D, Ghinolfi D, De Simone P et al (2015) Strategies to optimize the use of marginal donors in liver transplantation. World J Hepatol 7(26):2636–2647
Saidi RF (2013) Utilization of expanded criteria donors in liver transplantation. Int J Organ Transplant Med 4(2):46–59
Sotiropoulos GC, Paul A, Gerling T et al (2006) Liver transplantation with “rescue organ offers” within the eurotransplant area: a 2-year report from the University Hospital Essen. Transplantation 82(3):304–309
Doenecke A, Scherer MN, Tsui TY et al (2010) “Rescue allocation offers” in liver transplantation: is there any reason to reject “unwanted” organs? Scand J Gastroenterol 45(12):1516–1517
Mossdorf A, Kalverkamp S, Langenbrinck L et al (2013) Allocation procedure has no impact on patient and graft outcome after liver transplantation. Transpl Int 26(9):886–892
Schemmer P, Nickkholgh A, Gerling T et al (2009) Rescue allocation for liver transplantation within Eurotransplant: the Heidelberg experience. Clin Transplant 23(Suppl 21):42–48
Giretti G, Barbier L, Bucur P et al (2018) Recipient selection for optimal utilization of discarded grafts in liver transplantation. Transplantation 102(5):775–782
Ertel AE, Wima K, Hoehn RS et al (2015) Hospital utilization of nationally shared liver allografts from 2007 to 2012. World J Surg 40(4):958–966. https://doi.org/10.1007/s00268-015-3357-1
Halazun KJ, Quillin RC, Rosenblatt R et al (2017) Expanding the margins: high volume utilization of marginal liver grafts among > 2000 liver transplants at a single institution. Ann Surg 266(3):441–449
Marcon F, Schlegel A, Bartlett DC et al (2018) Utilization of declined liver grafts yields comparable transplant outcomes and previous decline should not be a deterrent to graft use. Transplantation 102(5):e211–e218
McCormack L, Quinonez E, Rios MM et al (2010) Rescue policy for discarded liver grafts: a single-centre experience of transplanting livers ‘that nobody wants’. HPB (Oxford) 12(8):523–530
Ravaioli M, Grazi GL, Cescon M et al (2009) Liver transplantations with donors aged 60 years and above: the low liver damage strategy. Transpl Int 22(4):423–433
Feng S, Goodrich NP, Bragg-Gresham JL et al (2006) Characteristics associated with liver graft failure: the concept of a donor risk index. Am J Transplant 6(4):783–790
Braat AE, Blok JJ, Putter H et al (2012) The Eurotransplant donor risk index in liver transplantation: ET-DRI. Am J Transplant 12(10):2789–2796
Dutkowski P, Oberkofler CE, Slankamenac K et al (2011) Are there better guidelines for allocation in liver transplantation? A novel score targeting justice and utility in the model for end-stage liver disease era. Ann Surg 254(5):745–753 discussion 753
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240(2):205–213
Olthoff KM, Kulik L, Samstein B et al (2010) Validation of a current definition of early allograft dysfunction in liver transplant recipients and analysis of risk factors. Liver Transplant 16(8):943–949
Lonjon G, Porcher R, Ergina P et al (2016) Potential pitfalls of reporting and bias in observational studies with propensity score analysis assessing a surgical procedure: a methodological systematic review. Ann Surg 265(5):901–909
Vandenbroucke JP, von Elm E, Altman DG et al (2007) Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Ann Intern Med 147(8):W163–W194
Ravaioli M, Grande G, Di Gioia P et al (2016) Risk avoidance and liver transplantation: a single-center experience in a national network. Ann Surg 264(5):778–786
Adam R, Bismuth H, Diamond T et al (1992) Effect of extended cold ischaemia with UW solution on graft function after liver transplantation. Lancet 340(8832):1373–1376
Stewart ZA, Locke JE, Segev DL et al (2009) Increased risk of graft loss from hepatic artery thrombosis after liver transplantation with older donors. Liver Transplant 15(12):1688–1695
Knight M, Barber K, Gimson A et al (2012) Implications of changing the minimal survival benefit in liver transplantation. Liver Transplant 18(5):549–557
Schaubel DE, Guidinger MK, Biggins SW et al (2009) Survival benefit-based deceased-donor liver allocation. Am J Transplant 9(4 Pt 2):970–981
Azoulay D, Audureau E, Bhangui P et al (2016) Living or brain-dead donor liver transplantation for hepatocellular carcinoma: a multicenter, western, intent-to-treat cohort study. Ann Surg 266(6):1035–1044
Battula NR, Platto M, Anbarasan R et al (2017) Intention to split policy: a successful strategy in a combined pediatric and adult liver transplant center. Ann Surg 265(5):1009–1015
Toso C, Ris F, Mentha G et al (2002) Potential impact of in situ liver splitting on the number of available grafts. Transplantation 74(2):222–226
Lai JC, Feng S, Roberts JP (2012) An examination of liver offers to candidates on the liver transplant wait-list. Gastroenterology 143(5):1261–1265
Edwards EB, Roberts JP, McBride MA et al (1999) The effect of the volume of procedures at transplantation centers on mortality after liver transplantation. N Engl J Med 341(27):2049–2053
Mirza DF, Gunson BK, Da Silva RF et al (1994) Policies in Europe on “marginal quality” donor livers. Lancet 344(8935):1480–1483
Morche J, Mathes T, Pieper D (2016) Relationship between surgeon volume and outcomes: a systematic review of systematic reviews. Syst Rev 5(1):204
Ozhathil DK, Li YF, Smith JK et al (2011) Impact of center volume on outcomes of increased-risk liver transplants. Liver Transplant 17(10):1191–1199
Acknowledgements
M.D. collected the data, interpreted the data, and wrote the manuscript. A.W. and C.G.G. performed the statistical analysis. H.H. interpreted the data and critically revised the manuscript. C.L. and C.S. interpreted the data and critically revised the manuscript. E.L. interpreted the data and critically revised the manuscript. C.F. interpreted the data and critically revised the manuscript. D.A. conceived the study, interpreted the data, and revised the manuscript. P.C. designed the study, interpreted the data, and wrote the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors of this manuscript have no conflict of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Azoulay, D., Disabato, M., Gomez-Gavara, C. et al. Liver Transplantation with “Hors Tour” Allocated Versus Standard MELD Allocated Grafts: Single-Center Audit and Impact on the Liver Pool in France. World J Surg 44, 912–924 (2020). https://doi.org/10.1007/s00268-019-05271-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-019-05271-w