
Abstract
Background
Operating room (OR) turnover time, time taken between one patient leaving the OR and the next entering, is an important determinant of OR utilization, a key value metric for hospital administrators. Surgical robots have increased the complexity and number of tasks required during an OR turnover, resulting in highly variable OR turnover times. We sought to streamline the turnover process and decrease robotic OR turnover times and increase efficiency.
Methods
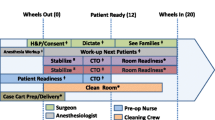
Direct observation of 45 pre-intervention robotic OR turnovers was performed. Following a previously successful model for handoffs, we employed concepts from motor racing pit stops, including briefings, leadership, role definition, task allocation and task sequencing. Turnover task cards for staff were developed, and card assignments were distributed for each turnover. Forty-one cases were observed post-intervention.
Results
Average total OR turnover time was 99.2 min (95% CI 88.0–110.3) pre-intervention and 53.2 min (95% CI 48.0–58.5) at 3 months post-intervention. Average room ready time from when the patient exited the OR until the surgical technician was ready to receive the next patient was 42.2 min (95% CI 36.7–47.7) before the intervention, which reduced to 27.2 min at 3 months (95% CI 24.7–29.7) post-intervention (p < 0.0001).
Conclusions
Role definition, task allocation and sequencing, combined with a visual cue for ease-of-use, create efficient, and sustainable approaches to decreasing robotic OR turnover times. Broader system changes are needed to capitalize on that result. Pit stop and other high-risk industry models may inform approaches to the management of tasks and teams.



Similar content being viewed by others

References
Cima RR, Brown MJ, Hebl JR et al (2011) Use of lean and six sigma methodology to improve operating room efficiency in a high-volume tertiary-care academic medical center. J Am Coll Surg 213:83–92 (discussion 93–84)
Donham RTBM, Hebl JR et al (1997) Glossary of times used for scheduling and monitoring of diagnostic and therapeutic procedures. AORN J 66(601–60):6
Tyler DC, Pasquariello CA, Chen CH (2003) Determining optimum operating room utilization. Anesth Analg 96:1114–1121 (table of contents)
Rebuck DA, Zhao LC, Helfand BT et al (2011) Simple modifications in operating room processes to reduce the times and costs associated with robot-assisted laparoscopic radical prostatectomy. J Endourol/Endourol Soc 25:955–960
Urrego H, Sanni A, Toro JP et al (2014) Out by 3: 30—a study in robotic bariatric surgery efficiency. Bariatr Surg Pract P 9:55–60
Stahl JE, Sandberg WS, Daily B et al (2006) Reorganizing patient care and workflow in the operating room: a cost-effectiveness study. Surgery 139:717–728
Anger JT, Mueller ER, Tarnay C et al (2014) Robotic compared with laparoscopic sacrocolpopexy: a randomized controlled trial. Obstet Gynecol 123:5–12
Nayeemuddin M, Daley SC, Ellsworth P (2013) Modifiable factors to decrease the cost of robotic-assisted procedures. AORN J 98:343–352
Catchpole KR, de Leval MR, McEwan A et al (2007) Patient handover from surgery to intensive care: using Formula 1 pit-stop and aviation models to improve safety and quality. Paediatr Anaesth 17:470–478
Funding
National Institute of Biomedical Imaging and Bioengineering (1R03EB017447, Catchpole/Anger).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr. Catchpole has no direct conflicts of interest to disclose; however, he has received research funding from Medtronic Ltd, and received funding to attend a meeting unrelated to this Project at Intuitive Surgical headquarters. Drs. Eilber and Anger have no direct conflicts of interest to disclose; however, they are investigators for ASTORA Women’s Health LLC, and investigators and expert witnesses for Boston Scientific Corporation. Drs. Souders, Wood, Solnik, and Strauss and Ray Avenido, RN have no conflicts of interest to disclose.
Rights and permissions
About this article

Cite this article
Souders, C.P., Catchpole, K.R., Wood, L.N. et al. Reducing Operating Room Turnover Time for Robotic Surgery Using a Motor Racing Pit Stop Model. World J Surg 41, 1943–1949 (2017). https://doi.org/10.1007/s00268-017-3936-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-017-3936-4