
Abstract
Introduction
Focused parathyroidectomy in primary hyperparathyroidism (1°HPT) is possible with accurate preoperative localization and intraoperative PTH monitoring (IOPTH). The added benefit of multimodal imaging techniques for operative success is unknown.
Method
Patients with 1°HPT, who underwent parathyroidectomy in 2012–2014 at a single institution, were retrospectively reviewed. Only the patients who underwent the standardized multimodal imaging workup consisting of 123I/99Tc-sestamibi subtraction scintigraphy, SPECT, and SPECT/CT were assessed.
Results
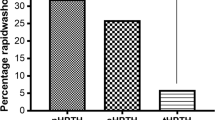
Of 360 patients who were identified, a curative operation was performed in 96 %, using pre-operative imaging and IOPTH. Imaging analysis showed that 123I/99Tc-sestamibi had a sensitivity of 86 % (95 % CI 82–90 %), positive predictive value (PPV) 93 %, and accuracy 81 %, based on correct lateralization. SPECT had a sensitivity of 77 % (95 % CI 72–82 %), PPV 92 % and accuracy 72 %. SPECT/CT had a sensitivity of 75 % (95 % CI 70–80 %), PPV of 94 %, and accuracy 71 %. There were 3 of 45 (7 %) patients with negative sestamibi imaging that had an accurate SPECT and SPECT/CT. Of 312 patients (87 %) with positive uptake on sestamibi (93 % true positive, 7 % false positive), concordant findings were present in 86 % SPECT and 84 % SPECT/CT. In cases where imaging modalities were discordant, but at least one method was true-positive, 123I/99Tc-sestamibi was significantly better than both SPECT and SPECT/CT (p < 0.001). The inclusion of SPECT and SPECT/CT in 1°HPT imaging protocol increases patient cost up to 2.4-fold.
Conclusion
123I/99Tc-sestamibi subtraction imaging is highly sensitive for preoperative localization in 1°HPT. SPECT and SPECT/CT are commonly concordant with 123I/99Tc-sestamibi and rarely increase the sensitivity. Routine inclusion of multimodality imaging technique adds minimal clinical benefit but increases cost to patient in high-volume setting.

Similar content being viewed by others


References
Mandl F (1926) Therapeutisher versuch bein falls von ostitis fibrosa generalisata mittles. Extirpation eines epithelkörperchen tumors. Wien Klin Wochenshr Zentral 143:245–284
van Heerden JA, Beahrs OH, Woolner LB (1977) The pathology and surgical management of primary hyperparathyroidism. Surg Clin N Am 57(3):557–563
Felger EA, Kandil E (2010) Primary hyperparathyroidism. Oto Clinic North Am 43(2):417–432
Shaha AR, Sarkar S, Strashun A et al (1997) Sestamibi scan for preoperative localization for primary hyperparathyroidism. Head Neck 19:87–91
Coakley AJ, Kettle AG, Wells CP et al (1989) 99Tm sestamibi—a new agent for parathyroid imaging. Nucl Med Commun 10(11):791–794
Grant CS, Thompson GB, Farley DR et al (2005) Primary hyperparathyroidism surgical management since the introduction of minimally invasive parathyroidectomy. Arch Surg 140:472–479
Udelsman R (2002) Six hundred fifty-six consecutive explorations for primary hyperparathyroidism. Ann Surg 235(5):665–672
Sharma J, Mazzaglia P, Milas M et al (2006) Radionuclide imaging for hyperparathyroidism (HPT): which is the best technetium-99 m sestamibi modality? Surgery 140:856–865
Richards ML, Thompson GB, Farley DR et al (2011) An optimal algorithm for intraoperative parathyroid hormone monitoring. Arch Surg 146(3):280–285
Sager S, Shafipour H, Asa S et al (2014) Comparison of Tc-99 m pertechnetate images with dual-phase Tc 99 m MIBI and SPECT images in primary hyperparathyroidism. IJEM 18(4):531–536
Neumann DR, Obuchowski NA, DiFilippo FP (2008) Preoperative 123I/99 m Tc-Sestamibi subtraction SPECT and SPECT/CT in primary hyperparathyroidism. J Nucl Med 49:2012–2017
Lavely WC, Friedman KP et al (2007) Comparison of SPECT/CT, SPECT, and planar imaging with single-and dual-phase 99mTc-Sestamibi parathyroid scintigraphy. J Nucl Med 48:1084–1089
Gayed IW, Kim EE, Broussard WF (2005) The value of 99mTc-Sestamibi SPECT/CT over conventional SPECT in the evaluation of parathyroid adenomas or hyperplasia. J Nucl Med 46:248–252
Tokmak H, Demirkol MO, Alagol F et al (2014) Clinical impact of SPECT-CT in the diagnosis and surgical management of hyperparathyroidism. Int J Clin Exp Med 7(4):1028–1034
Rubello D, Gross MD, Mariani G et al (2007) Scintigraphic techniques in primary hyperparathyroidism: from pre-operative localization to intra-operative imaging. Eur J Nucl Med Mol Imaging 34:926–933
Pham TH, Sylvester Sterioff S, Mullan BP et al (2006) Sensitivity and utility of parathyroid scintigraphy in patients with primary versus secondary and tertiary hyperparathyroidism. World J Surg 30:327–332
Shin JJ, Milas M, Mitchell J et al (2011) Impact of localization studies and clinical scenario in patients with hyperparathyroidism being evaluated for reoperative neck surgery. Arch Surg 146(12):1397–1403
Yen TW, Wang TS, Doffek KM et al (2008) Reoperative parathyroidectomy: an algorithm for imaging and monitoring of intraoperative parathyroid hormone levels that results in successful focused approach. Surgery 144:611–621
Richards ML, Thompson GB, Farley DR et al (2008) Reoperative parathyroidectomy in 228 patients during the era of minimal-access surgery and intraoperative parathyroid hormone monitoring. Am J Surg 196:937–943
Dy BM, Richards ML, Vazquez BJ et al (2012) Primary hyperparathyroidism and negative Tc99 Sestamibi Imaging: to operate or not? Ann Surg Oncol 19:2272–2278
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest to disclose.
Rights and permissions
About this article

Cite this article
Lee, G.S., McKenzie, T.J., Mullan, B.P. et al. A Multimodal Imaging Protocol, 123I/99Tc-Sestamibi, SPECT, and SPECT/CT, in Primary Hyperparathyroidism Adds Limited Benefit for Preoperative Localization. World J Surg 40, 589–594 (2016). https://doi.org/10.1007/s00268-015-3389-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-015-3389-6