
Abstract
Background
Adrenal cortical carcinoma (ACC) may have tumor or patient characteristics at presentation that argue against immediate surgery because of an unacceptable risk of morbidity/mortality, incomplete resection, or recurrence. This clinical stage can be characterized as borderline resectable ACC (BRACC). At present, systemic therapies in ACC can reduce tumor burden in some patients, creating an opportunity in BRACC for a strategy of preoperative chemotherapy (ctx) followed by surgery.
Materials and Methods
A single-institution retrospective review was conducted of all patients considered for surgery for primary ACC. Patients with BRACC treated with preoperative ctx were categorized as follows: group A, imaging suggesting a need for multiorgan/vascular resection; group B, imaging suggesting potentially resectable oligometastases; and group C, patients having marginal performance status/comorbidities precluding immediate surgery. Both the disease-free survival (DFS) and the overall survival (OS) were compared in BRACC patients treated with preoperative ctx+surgery and those who had upfront surgery.
Results
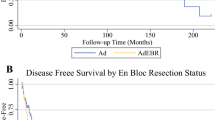
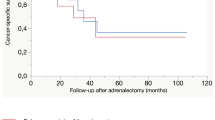
Fifty-three patients with primary ACC were considered for surgery (median follow-up: 49.9 months). Thirty-eight patients (71.7 %) had initial surgery and 15 of them (28.3 %) were considered BRACC and received preoperative therapy. Of these 15 patients, 12 (80 %) received combination therapy with mitotane and etoposide/cisplatin-based ctx, 2 (13 %) received mitotane alone, and 1 (7 %) received ctx alone. Six patients were defined as group A, 5 as group B, and 4 as group C. Thirteen (87 %) BRACC patients underwent surgical resection. BRACC patients were younger but had more advanced disease than the patients having initial surgery (stage IV in 40 vs 2.6 % [p < 0.01]). By Response Evaluation Criteria In Solid Tumors criteria, 5 patients (38.5 %) had a partial response, 7 (53.8 %) had stable disease, and 1 (7.7 %) had disease that progressed. Postoperative mitotane use was similar between groups (p = .15). Median DFS for resected BRACC patients was 28.0 months [95 % confidence interval (CI), 2.9–not attained] vs 13 months (95 % CI, 5.8–46.9) (p = 0.40) for initial surgery patients. Five-year OS rates were also similar: 65 % for resected BRACC vs 50 % for initial surgery (p = 0.72).
Conclusions
The favorable outcome of patients with BRACC, despite more advanced stage of disease compared to those treated with surgery first, together with uncommon disease progression, suggests a benefit of neoadjuvant treatment sequencing in patients with BRACC.




Similar content being viewed by others

References
Fassnacht M, Johanssen S, Quinkler M et al (2009) Limited prognostic value of the 2004 international union against cancer staging classification for adrenocortical carcinoma: proposal for a revised TNM classification. Cancer 115:243–250
Maluf DF, de Oliveira BH, Lalli E (2011) Therapy of adrenocortical cancer: present and future. Am J Cancer Res 1:222–232
Kerkhofs TM, Verhoeven RH, Van der Zwan JM et al (2013) Adrenocortical carcinoma: a population-based study on incidence and survival in the Netherlands since 1993. Eur J Cancer 49:2579–2586
Stigliano A, Cerquetti L, Sampaoli C et al (2012) Current and emerging therapeutic options in adrenocortical cancer treatment. J Oncol 2012:408131
Grubbs EG, Callender GG, Xing Y et al (2010) Recurrence of adrenal cortical carcinoma following resection: surgery alone can achieve results equal to surgery plus mitotane. Ann Surg Oncol 17:263–270
Terzolo M, Angeli A, Fassnacht M et al (2007) Adjuvant mitotane treatment for adrenocortical carcinoma. N Engl J Med 356:2372–2380
Fassnacht M, Terzolo M, Allolio B et al (2012) Combination chemotherapy in advanced adrenocortical carcinoma. N Engl J Med 366:2189–2197
Katz MH, Pisters PW, Evans DB et al (2008) Borderline resectable pancreatic cancer: the importance of this emerging stage of disease. J Am Coll Surg 206:833–846 discussion 846–848
Tempero MA, Arnoletti JP, Behrman S et al (2010) Pancreatic adenocarcinoma. J Natl Compr Cancer Netw 8:972–1017
Lughezzani G, Sun M, Perrotte P et al (2010) The European network for the study of adrenal tumors staging system is prognostically superior to the international union against cancer-staging system: a North American validation. Eur J Cancer 46:713–719
Therasse P, Arbuck SG, Eisenhauer EA et al (2000) New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Compr Cancer Netw 92:205–216
Bourdeau I, Mackenzie-Feder J, Lacroix A (2013) Recent advances in adrenocortical carcinoma in adults. Curr Opin Endocrinol Diabetes Obes 20:192–197
Zini L, Porpiglia F, Fassnacht M (2011) Contemporary management of adrenocortical carcinoma. Eur Urol 60:1055–1065
Gonzalez RJ, Tamm EP, Ng C et al (2007) Response to mitotane predicts outcome in patients with recurrent adrenal cortical carcinoma. Surgery 142:867–875 discussion 875
Abrams RA, Lowy AM, O’Reilly EM et al (2009) Combined modality treatment of resectable and borderline resectable pancreas cancer: expert consensus statement. Ann Surg Oncol 16:1751–1756
Evans DB, Farnell MB, Lillemoe KD et al (2009) Surgical treatment of resectable and borderline resectable pancreas cancer: expert consensus statement. Ann Surg Oncol 16:1736–1744
Vauthey JN, Dixon E (2009) AHPBA/SSO/SSAT consensus conference on resectable and borderline resectable pancreatic cancer: rationale and overview of the conference. Ann Surg Oncol 16:1725–1726
Berruti A, Fassnacht M, Baudin E et al (2010) Adjuvant therapy in patients with adrenocortical carcinoma: a position of an international panel. J Clin Oncol 28:e401–e402 author reply e3
Datrice NM, Langan RC, Ripley RT et al (2012) Operative management for recurrent and metastatic adrenocortical carcinoma. J Surg Oncol 105:709–713
Gaujoux S, Al-Ahmadie H, Allen PJ et al (2012) Resection of adrenocortical carcinoma liver metastasis: is it justified? Ann Surg Oncol 19:2643–2651
Kemp CD, Ripley RT, Mathur A et al (2011) Pulmonary resection for metastatic adrenocortical carcinoma: the National Cancer Institute experience. Ann Thorac Surg 92:1195–1200
Hermsen IG, Kerkhofs TM, den Butter G et al (2012) Surgery in adrenocortical carcinoma: importance of national cooperation and centralized surgery. Surgery 152:50–56
Miller BS, Gauger PG, Hammer GD et al (2012) Resection of adrenocortical carcinoma is less complete and local recurrence occurs sooner and more often after laparoscopic adrenalectomy than after open adrenalectomy. Surgery 152:1150–1157
Disclosures
The authors have no disclosures.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bednarski, B.K., Habra, M.A., Phan, A. et al. Borderline Resectable Adrenal Cortical Carcinoma: A Potential Role for Preoperative Chemotherapy. World J Surg 38, 1318–1327 (2014). https://doi.org/10.1007/s00268-014-2484-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-014-2484-4