
Abstract
Background
The benefit of adrenalectomy (ADX) for adrenal metastasis is not established. We evaluated outcomes after ADX for patients with adrenal metastasis.
Methods
We retrospectively analyzed the records of 90 patients who underwent ADX for metastatic disease. Overall survival (OS) after ADX was calculated using the Kaplan–Meier method. Clinical factors were evaluated for associations with OS using a Cox regression model, and with operative factors using the Wilcoxon two-sample or Fisher’s exact test.
Results
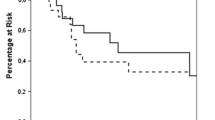
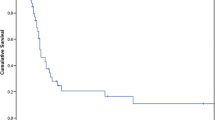
The most common primary tumor types were melanoma (35, 39 %) and lung cancer (32, 35 %). A total of 49 (54 %) patients had isolated adrenal metastasis; 55 (61 %) underwent laparoscopic resection (LADX). Median OS was 2.46 years (range < 1 month–15 years), and 5-year survival rate was 38 % (6 % standard error). Most patients experienced disease progression (56, 62 %) despite achieving disease-free status following ADX (78, 86 %). When compared with the open approach, LADX was associated with smaller tumor size, as well as reduced blood loss, operative time, and length of stay (all p < 0.0001), and no difference in OS (p = 0.4122) or complications (p = 1). Isolated adrenal bed recurrence was similar in LADX (N = 3, 5 %) and open ADX (N = 2, 6 %) (p = 1), and did not affect OS (p = 0.2). Larger tumors were associated with shorter median OS (p = 0.0014).
Conclusions
ADX for metastasis can be safely performed in selected patients. Some patients with adrenal metastasis achieve prolonged survival following ADX. Compared with an open approach, LADX has no measurable oncologic disadvantage, minimizes morbidity, and should be considered when tumor characteristics permit.



Similar content being viewed by others

References
Abrams HL, Spiro R, Goldstein N (1950) Metastases in carcinoma: analysis of 1000 autopsied cases. Cancer 3(1):74–85
Lo CY, VanHeerden JA, Soreide JA et al (1996) Adrenalectomy for metastatic disease to the adrenal glands. Br J Surg 83:528–531
Lam KY, Lo CY (2002) Metastatic tumours of the adrenal glands: a 30-year experience in a teaching hospital. Clin Endocrinol 56:95–101
Aron D, Terzolo M, Cawood TJ (2012) Adrenal incidentalomas. Best Pract Res Clin Endocrinol Metab 26:69–82
No authors listed (2002) NIH state-of-the-science statement on management of the clinically inapparent adrenal mass (“Incidentaloma”) NIH Consens State Sci Statements 19(2):1–23
Lenert JE, Barnett CC, Kudelka AP et al (2001) Evaluation and surgical resection of adrenal masses in patients with a history of extra-adrenal malignancy. Surgery 130:1060–1067
Zeiger MA, Thompson GB, Duh QY et al (2009) AACE/AAES adrenal incidentaloma guidelines. Endocr Pract 15(5):450–453
Mittendorf EA, Lim SJ, Schacherer CW et al (2008) Melanoma adrenal metastasis: natural history and surgical management. Am J Surg 195:363–369
Vazquez BJ, Richards ML, Lohse CM et al (2012) Adrenalectomy improves outcomes of selected patients with metastatic carcinoma. World J Surg 36:1400–1405
Moreno P, de la Quintana Basarrate A, Musholt TJ et al (2013) Adrenalectomy for solid tumor metastases: results of a multicenter European study. Abstract presented at American Association of Endocrine Surgeons, Chicago (IL), April 14
Heniford BT, Arca MJ, Walsh RM et al (1999) Laparoscopic adrenalectomy for cancer. Semin Surg Onc 16:293–306
Luketich JD, Burt ME (1996) Does resection of adrenal metastases from non-small cell lung cancer improve survival? Ann Thorac Surg 63:1614–1616
Strong VE, D’angelica M, Tang L et al (2007) Laparoscopic adrenalectomy for isolated adrenal metastasis. Annals Surg Onc 14:3392–3400
Perrier ND, Kennamer DL, Bao R et al (2008) Posterior retroperitoneoscopic adrenalectomy: preferred technique for removal of benign tumors and isolated metastases. Annals Surg 248:666–674
Acknowledgments
The authors would like to thank Mr. Roland Bassett for his assistance on the statistical analysis and Ms. Melissa Burkett for editorial assistance in manuscript preparation.
Conflict of interest
The authors have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Romero Arenas, M.A., Sui, D., Grubbs, E.G. et al. Adrenal Metastectomy is Safe in Selected Patients. World J Surg 38, 1336–1342 (2014). https://doi.org/10.1007/s00268-014-2454-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-014-2454-x