
Abstract
Background
The World Health Organization has identified the primary referral hospital as its priority site for improving surgical care in low- and middle-income countries. Little is known about the relative burden surgical patients place on health care facilities at this level. This research estimates the fraction of admissions due to surgical conditions at three hospitals in rural Mozambique.
Methods
Prospective data were collected on all inpatients at three primary referral hospitals in Mozambique during a 12-day period. We compared the number of surgical patients and their length of stay (LOS) to the patients admitted to the medicine, pediatric, and maternity wards. These findings were validated using retrospective data collected from one hospital from January to May 2012.
Results
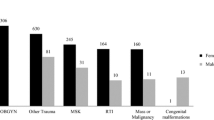
Patients with surgical conditions (i.e., patients admitted to the surgical or maternity ward) accounted for 57.5 % of admissions and 48.0 % of patient-days. The majority of patients were admitted to the maternity ward (32.3 %). The other admissions were evenly distributed to the pediatric (22.5 %), medical (20.0 %), and surgical (25.2 %) wards. Compared to patients from the three other wards, surgical patients had longer average LOS (8.7 vs. 1.9–7.7 days) and a higher number of total patient-days (891 vs. 252–703 days). The most prevalent procedures were cesarean section (33.3 %) and laceration repair/wound care (11.8 %).
Conclusions
Surgical conditions are the most common reason for admissions at three primary referral hospitals in rural Mozambique. These data suggest that surgical care is a major component of health care delivered at primary referral hospitals in Mozambique and likely other sub-Saharan African countries.



Similar content being viewed by others

References
Debas HT, Gosselin R, McCord C et al (2006) Surgery. In: Jamison DT, Breman JG, Measham AR et al (eds) Disease control priorities in developing countries, 2nd edn. The International Bank for Reconstruction and Development/The World Bank Group, Washington
Mathers CD, Loncar D (2006) Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med 3:e442
Weiser TG, Regenbogen SE, Thompson KD et al (2008) An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet 372:139–144
Ozgediz D, Jamison D, Cherian M et al (2008) The burden of surgical conditions and access to surgical care in low- and middle-income countries. Bull World Health Organ 86:646–647
Farmer PE, Kim JY (2008) Surgery and global health: a view from beyond the OR. World J Surg 32:533–536. doi:10.1007/s00268-008-9525-9
Atiyeh BS, Gunn SW, Hayek SN (2010) Provision of essential surgery in remote and rural areas of developed as well as low and middle income countries. Int J Surg 8:581–585
UNDP (2011) Human development report 2011: sustainability and equity—a better future for all. Palgrave Macmillan, New York
The World Bank (2011) World development indicators. The World Bank, Washington
USAID (2006) Health sector (SO8) overview: briefing book. http://transition.usaid.gov/mz/doc/misc/health%20overview_nov2006.pdf. Accessed 1 May 2013
Lindelow M (2002) Health care demand in rural Mozambique: evidence from the 1996/97 household survey. http://www.ifpri.org/publication/health-care-demand-rural-mozambique-0. Accessed 1 May 2013
Bickler S, Ozgediz D, Gosselin R et al (2010) Key concepts for estimating the burden of surgical conditions and the unmet need for surgical care. World J Surg 34:374–380. doi:10.1007/s00268-009-0261-6
Galukande M, von Schreeb J, Wladis A et al (2010) Essential surgery at the district hospital: a retrospective descriptive analysis in three African countries. PLoS Med 7:e1000243
Notrica MR, Evans FM, Knowlton LM et al (2011) Rwandan surgical and anesthesia infrastructure: a survey of district hospitals. World J Surg 35:1770–1780. doi:10.1007/s00268-011-1125-4
Kushner AL, Cherian MN, Noel L et al (2010) Addressing the millennium development goals from a surgical perspective: essential surgery and anesthesia in 8 low- and middle-income countries. Arch Surg 145:154–159
Williams BG, Lloyd-Smith JO, Gouws E et al (2006) The potential impact of male circumcision on HIV in sub-Saharan Africa. PLoS Med 3:e262
Laxminarayan R, Chow J, Shahid-Salles SA (2006) Intervention cost-effectiveness: overview of main messages. In: Jamison DT, Breman JG, Measham AR (eds) Disease control priorities in developing countries, 2nd edn. The International Bank for Reconstruction and Development/The World Bank Group, Washington
Luboga S, Macfarlane SB, von Schreeb J et al (2009) Increasing access to surgical services in sub-saharan Africa: priorities for national and international agencies recommended by the Bellagio Essential Surgery Group. PLoS Med 6:e1000200
UNAIDS (2012) Global report: UNAIDS report on the global AIDS epidemic. http://www.unaids.org/globalreport/global_report.htm. Accessed 1 May 2013
Acknowledgments
The research was supported by Grant No. R24TW008910 from the Fogarty International Center. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Fogarty International Center or the National Institutes of Health. The NIH Common Fund supports the first award.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Anderson, J.E., Erickson, A., Funzamo, C. et al. Surgical Conditions Account for the Majority of Admissions to Three Primary Referral Hospitals in Rural Mozambique. World J Surg 38, 823–829 (2014). https://doi.org/10.1007/s00268-013-2366-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-013-2366-1