
Abstract
Background
The incidence of internal hernia after gastrectomy can increase with the increasing use of laparoscopic surgery, although this trend has not been elucidated.
Methods
Clinical information was collected from medical records and by questionnaire for 18 patients who underwent surgical treatment for internal hernia after gastrectomy for gastric cancer in 24 hospitals from January 2005 to December 2009.
Results
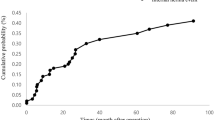
Gastrectomy for gastric cancer was open/distal gastrectomy (DG) in five (28%) patients, open/total gastrectomy (TG) in seven (39%), laparoscopy-assisted/DG in three (17%), and laparoscopy-assisted/TG in 3 (17%). Reconstruction was by Roux-Y methods in all patients. The hernia orifice was classified as a jejunojejunostomy mesenteric defect in eight patients (44%), dorsum of the Roux limb (Petersen’s space) in eight (44%), and one (5%) each of esophageal hiatus and mesenterium of the transverse colon. Among 8,983 patients who underwent gastrectomy for gastric cancer, a postoperative survey revealed that 13 patients underwent surgical treatment for internal hernia in the same hospitals. The 3-year incidence rate of the internal hernia was 0.19%, which was significantly higher after laparoscopy-assisted than open gastrectomy (0.53 vs. 0.15%, p = 0.03). Patients with an internal hernia had a mean (±SD) low weight at hernia operation (body mass index 17.9 ± 1.6 kg/m2) and marked weight loss after gastrectomy (weight reduction 15.6 ± 5.8%).
Conclusions
Gastrectomy with Roux-Y reconstruction for gastric cancer leaves several spaces that can cause internal hernia formation. Laparoscopic surgery and postoperative body weight loss are potential risk factors.



Similar content being viewed by others

References
Ellis H, Moran BJ, Thompson JN et al (1999) Adhesion-related hospital readmissions after abdominal and pelvic surgery: a retrospective cohort study. Lancet 353:1476–1480
Menzies D, Ellis H (1990) Intestinal obstruction from adhesions: how big is the problem? Ann R Coll Surg Engl 72:60–63
Fevang BT, Fevang J, Stangeland L et al (2000) Complications and death after surgical treatment of small bowel obstruction: a 35-year institutional experience. Ann Surg 231:529–537
Sosa J, Gardner B (1993) Management of patients diagnosed as acute intestinal obstruction secondary to adhesions. Am Surg 59:125–128
Fazio VW, Cohen Z, Fleshman JW et al (2006) Reduction in adhesive small-bowel obstruction by Seprafilm adhesion barrier after intestinal resection. Dis Colon Rectum 49:1–11
Mohri Y, Uchida K, Araki T et al (2005) Hyaluronic acid-carboxycellulose membrane (Seprafilm) reduces early postoperative small bowel obstruction in gastrointestinal surgery. Am Surg 71:861–863
Gervaz P, Inan I, Perneger T et al (2010) A prospective, randomized, single-blind comparison of laparoscopic versus open sigmoid colectomy for diverticulitis. Ann Surg 252:3–8
Sharma B, Baxter N, Grantcharov T (2010) Outcomes after laparoscopic techniques in major gastrointestinal surgery. Curr Opin Crit Care 16:371–376
Rosin D, Zmora O, Hoffman A et al (2007) Low incidence of adhesion-related bowel obstruction after laparoscopic colorectal surgery. J Laparoendosc Adv Surg Tech A 17:604–607
Dowson HM, Bong JJ, Lovell DP et al (2008) Reduced adhesion formation following laparoscopic versus open colorectal surgery. Br J Surg 95:909–914
Capella RF, Iannace VA, Capella JF (2006) Bowel obstruction after open and laparoscopic gastric bypass surgery for morbid obesity. J Am Coll Surg 203:328–335
Hosono S, Ohtani H, Arimoto Y et al (2007) Internal hernia with strangulation through a mesenteric defect after laparoscopy-assisted transverse colectomy: report of a case. Surg Today 37:330–334
Ghahremani GG (1984) Internal abdominal hernias. Surg Clin N Am 64:393–406
Aoki M, Saka M, Morita S et al (2010) Afferent loop obstruction after distal gastrectomy with Roux-en-Y reconstruction. World J Surg 34:2389–2392
Gayer G, Barsuk D, Hertz M et al (2002) CT diagnosis of afferent loop syndrome. Clin Radiol 57:835–839
Education Committee of Japan Society for Endoscopic Surgery (2010) 10th Nationwide survey of endoscopic surgery in Japan. J Jpn Soc Endosc Surg J 15:567–577
Morita S, Sano T, Tanaka N et al (2010) Trends in reconstruction and anastomosis for patients with gastric cancer. Jpn J Cancer Clin 56:9–14
Csendes A, Burgos AM, Smok G et al (2009) Latest results (12–21 years) of a prospective randomized study comparing Billroth II and Roux-en-Y anastomosis after a partial gastrectomy plus vagotomy in patients with duodenal ulcers. Ann Surg 249:189–194
Kojima K, Yamada H, Inokuchi M et al (2008) A comparison of Roux-en-Y and Billroth-I reconstruction after laparoscopy-assisted distal gastrectomy. Ann Surg 247:962–967
Iannelli A, Facchiano E, Gugenheim J (2006) Internal hernia after laparoscopic Roux-en-Y gastric bypass for morbid obesity. Obes Surg 16:1265–1271
Comeau E, Gagner M, Inabnet WB et al (2005) Symptomatic internal hernias after laparoscopic bariatric surgery. Surg Endosc 19:34–39
Coleman MH, Awad ZT, Pomp A et al (2006) Laparoscopic closure of the Petersen mesenteric defect. Obes Surg 16:770–772
Bauman RW, Pirrello JR (2009) Internal hernia at Petersen’s space after laparoscopic Roux-en-Y gastric bypass: 6.2% incidence without closure—a single surgeon series of 1047 cases. Surg Obes Relat Dis 5:565–570
Miyashiro LA, Fuller WD, Ali MR (2010) Favorable internal hernia rate achieved using retrocolic, retrogastric alimentary limb in laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis 6:158–162
Steele KE, Prokopowicz GP, Magnuson T et al (2008) Laparoscopic antecolic Roux-en-Y gastric bypass with closure of internal defects leads to fewer internal hernias than the retrocolic approach. Surg Endosc 22:2056–2061
Davies J, Johnston D, Sue-Ling H et al (1998) Total or subtotal gastrectomy for gastric carcinoma? A study of quality of life. World J Surg 22:1048–1055
Tyrvainen T, Sand J, Sintonen H et al (2008) Quality of life in the long-term survivors after total gastrectomy for gastric carcinoma. J Surg Oncol 97:121–124
Nunobe S, Okaro A, Sasako M et al (2007) Billroth 1 versus Roux-en-Y reconstructions: a quality-of-life survey at 5 years. Int J Clin Oncol 12:433–439
Takiguchi S, Yamamoto K, Hirao M et al. (2011) A comparison of postoperative quality of life and dysfunction after Billroth I and Roux-en-Y reconstruction following distal gastrectomy for gastric cancer: results from a multi-institutional RCT. Gastric Cancer. doi:10.1007/s10120-011-0098-1
Muller MK, Rader S, Wildi S et al (2008) Long-term follow-up of proximal versus distal laparoscopic gastric bypass for morbid obesity. Br J Surg 95:1375–1379
Hope WW, Sing RF, Chen AY et al (2010) Failure of mesenteric defect closure after Roux-en-Y gastric bypass. JSLS 14:213–216
Miyato H, Kitayama J, Hidemura A et al (2010) Vagus nerve preservation selectively restores visceral fat volume in patients with early gastric cancer who underwent gastrectomy. J Surg Res. doi:10.1002/bjs.6453
Papasavas PK, Caushaj PF, McCormick JT et al (2003) Laparoscopic management of complications following laparoscopic Roux-en-Y gastric bypass for morbid obesity. Surg Endosc 17:610–614
Mathieu D, Luciani A (2004) Internal abdominal herniations. Am J Roentgenol 183:397–404
Takeyama N, Gokan T, Ohgiya Y et al (2005) CT of internal hernias. Radiographics 25:997–1015
Lockhart ME, Tessler FN, Canon CL et al (2007) Internal hernia after gastric bypass: sensitivity and specificity of seven CT signs with surgical correlation and controls. Am J Roentgenol 188:745–750
Krajewski S, Brown J, Phang PT et al (2011) Impact of computed tomography of the abdomen on clinical outcomes in patients with acute right lower quadrant pain: a meta-analysis. Can J Surg 54:43–53
Kothari SN (2011) Bariatric surgery and postoperative imaging. Surg Clin N Am 91:155–172
Hong SS, Kim AY, Kwon SB et al (2010) Three-dimensional CT enterography using oral Gastrografin in patients with small bowel obstruction: comparison with axial CT images or fluoroscopic findings. Abdom Imaging 35:556–562
Kawkabani Marchini A, Denys A, Paroz A et al (2011) The four different types of internal hernia occurring after laparoscopic Roux-en-Y gastric bypass performed for morbid obesity: are there any multidetector computed tomography (MDCT) features permitting their distinction? Obes Surg 21:506–516
Acknowledgments
This study was conducted without any financial support. The authors thank all participants of the Osaka University Clinical Research Group for Gastroenterological Surgery. The following is a list of the 24 high-volume centers in Kinki area that participated in this study: National Hospital Organization Osaka National Hospital, Osaka; Toyonaka Municipal Hospital, Osaka; Osaka Medical Center for Cancer and Cardiovascular Diseases, Osaka; Kansai Rosai Hospital, Hyogo; Osaka Police Hospital, Osaka; Osaka University Hospital, Osaka; Osaka General Medical Center, Osaka; Osaka Rosai Hospital, Osaka; Osaka Koseinenkin Hospital, Osaka; Nara Hospital Kinki University Faculty of Medicine, Nara; NTT West Osaka Hospital, Osaka; Higashiosaka City General Hospital, Osaka; Hyogo Prefectural Nishinomiya Hospital, Hyogo; Ikeda City Hospital, Osaka; Otemae Hospital, Osaka; Itami City Hospital, Hyogo; Bell Land General Hospital, Osaka; Moriguchi Keijinkai Hospital, Osaka; Social Insurance Kinan Hospital, Wakayama; Yao Municipal Hospital, Osaka; Kinki Central Hospital, Hyogo; Suita Municipal Hospital, Osaka; Minoh City Hospital, Osaka; Saiseikai Senri Hospital, Osaka, Japan.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Miyagaki, H., Takiguchi, S., Kurokawa, Y. et al. Recent Trend of Internal Hernia Occurrence After Gastrectomy for Gastric Cancer. World J Surg 36, 851–857 (2012). https://doi.org/10.1007/s00268-012-1479-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-012-1479-2