
Abstract
Background
Endoscopic thyroidectomies have been performed using various approaches, and indications have expanded with the development of new surgical techniques and instruments. Endoscopic thyroid surgery using bilateral axillo-breast approaches have excellent cosmetic results and a symmetrical, optimal operative view. However, because of the two-dimensional view and the nonflexible instruments, these approaches are not easy to use in performing a central lymph node dissection (CND). Robotic surgery has drawn attention as a potentially safe and effective method for treating thyroid cancer. The aim of the present study was to determine whether robotic surgery is superior to endoscopic and open surgery through comparing technical aspects and surgical outcomes.
Methods
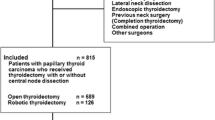
From October 2008 to December 2009, 302 patients had total thyroidectomies and CND with cancer less than 1 cm. Patients were divided into three groups according to operation methods (open group; n = 138), (endo group; n = 95), (robot group; n = 69).
Results
Young patients preferred the robotic and endoscopic surgery. The number of retrieved lymph nodes in the open group (4.8 ± 2.8) was not different from the robot group (4.7 ± 2.7) and the endo group (4.6 ± 3.7). The operative time of the robot group was longer than the open and the endo group. The total drain amount in the robot group was more than the open and endo groups; however, there was no difference in the length of hospitalization and complication rates. There were no differences between the open (0.8 ± 2.0) and robot groups (0.8 ± 1.4), but the endo group (2.4 ± 6.3) showed higher postoperative serum thyroglobulin off thyroid hormone (Off-Tg) when compared to the open and robot groups.
Conclusions
Robotic surgery was equal to open surgery except with respect to operative time and was superior to endoscopic surgery in Off-Tg levels presenting completeness of the operation in thyroid cancer surgery. Because it has excellent cosmetic results and various technical advantages, it should be considered in young, low-risk patients with thyroid carcinoma less than 1 cm.


Similar content being viewed by others


References
Huscher CS, Chiodini S, Napolitano C et al (1997) Endoscopic right thyroid lobectomy. Surg Endosc 11:877
Kitano H, Fujimura M, Kinoshita T et al (2002) Endoscopic thyroid resection using cutaneous elevation in lieu of insufflation. Surg Endosc 16:88–91
Ikeda Y, Takami H, Niimi M et al (2001) Endoscopic thyroidectomy by the axillary approach. Surg Endosc 15:1362–1364
Ohgami M, Ishii S, Arisawa Y et al (2000) Scarless endoscopic thyroidectomy: breast approach for better cosmesis. Surg Laparosc Endosc Percutan Tech 10:1–4
Shimazu K, Shiba E, Tamaki Y et al (2003) Endoscopic thyroid surgery through the axillo-bilateral-breast approach. Surg Laparosc Endosc Percutan Tech 13:196–201
Chung YS, Choe JH, Kang KH et al (2007) Endoscopic thyroidectomy for thyroid malignancies: comparison with conventional open thyroidectomy. World J Surg 31:2302–2306 discussion 2307–2308
Jeong JJ, Kang SW, Yun JS et al (2009) Comparative study of endoscopic thyroidectomy versus conventional open thyroidectomy in papillary thyroid microcarcinoma (PTMC) patients. J Surg Oncol 100:477–480
Ikeda Y, Takami H, Sasaki Y et al (2002) Comparative study of thyroidectomies. Endoscopic surgery versus conventional open surgery. Surg Endosc 16:1741–1745
Choe JH, Kim SW, Chung KW et al (2007) Endoscopic thyroidectomy using a new bilateral axillo-breast approach. World J Surg 31:601–606
Tanna N, Joshi AS, Glade RS et al (2006) Da Vinci robot-assisted endocrine surgery: novel applications in otolaryngology. Otolaryngol Head Neck Surg 135:633–635
Lee KE, Rao J, Youn YK (2009) Endoscopic thyroidectomy with the da Vinci robot system using the bilateral axillary breast approach (BABA) technique: our initial experience. Surg Laparosc Endosc Percutan Tech 19:e71–e75
Kang SW, Jeong JJ, Yun JS et al (2009) Robot-assisted endoscopic surgery for thyroid cancer: experience with the first 100 patients. Surg Endosc 23:2399–2406
Yoon JH, Park CH, Chung WY (2006) Gasless endoscopic thyroidectomy via an axillary approach: experience of 30 cases. Surg Laparosc Endosc Percutan Tech 16:226–231
Ikeda Y, Takami H, Sasaki Y et al (2000) Endoscopic resection of thyroid tumors by the axillary approach. J Cardiovasc Surg (Torino) 41:791–792
Ikeda Y, Takami H, Sasaki Y et al (2000) Endoscopic neck surgery by the axillary approach. J Am Coll Surg 191:336–340
Miccoli P, Elisei R, Materazzi G et al (2002) Minimally invasive video-assisted thyroidectomy for papillary carcinoma: a prospective study of its completeness. Surgery 132:1070–1073 discussion 1073–1074
Miccoli P, Berti P, Raffaelli M et al (2001) Comparison between minimally invasive video-assisted thyroidectomy and conventional thyroidectomy: a prospective randomized study. Surgery 130:1039–1043
Link RE, Bhayani SB, Kavoussi LR (2006) A prospective comparison of robotic and laparoscopic pyeloplasty. Ann Surg 243:486–491
Randolph GW (2003) Surgery of the thyroid and parathyroid glands. W. B. Saunders, Philadelphia, pp 434–439
Cooper DS, Doherty GM, Haugen BR et al (2009) Revised American thyroid association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 19:1167–1214
Author information
Authors and Affiliations
Corresponding author
Additional information
Wan Wook Kim and Jee Soo Kim contributed equally to this work.
Rights and permissions
About this article
Cite this article
Kim, W.W., Kim, J.S., Hur, S.M. et al. Is Robotic Surgery Superior to Endoscopic and Open Surgeries in Thyroid Cancer?. World J Surg 35, 779–784 (2011). https://doi.org/10.1007/s00268-011-0960-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-011-0960-7