
Abstract
Background
Up to 30% of surgical inpatients develop complications related to fluid and electrolyte therapy. We sought to study the occurrence of hypo- and hypernatraemia in these patients to inform current standards of care.
Methods
This prospective audit took place over 80 days in a university hospital. Patients with a serum sodium concentration less than 130 or greater than 150 mmol/l were included. Daily intakes of Na+, K+ and Cl−, and fluid balance were recorded before and after development of dysnatraemia. Fluid balance charts were assessed, as was the presence of documented patient weights. Patients were followed up until one of these milestones was reached: normonatraemia, death, or hospital discharge.
Results
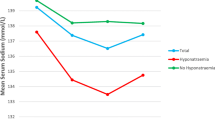
During the study period 55 (4%) of the 1,383 surgical admissions met the inclusion criteria. Fifteen patients had hypernatraemia, 13 (87%) of whom were identified on ICU/HDU. In the days preceding the hypernatraemia, patients received (in mmol/day) a median (IQR) of 157 (76–344) Na+, 38 (6–65) K+, 157 (72–310) Cl−, and 1.96 (1.13–2.96) L water. In the days preceding the hyponatraemia, patients received 50 (0–189) Na+, 0 (0–10) K+, 56 (0–188) Cl−, and 1.45 (0–2.60) L water. Before the dysnatraemias only 28% of fluid balance charts were completed accurately. During the audit 42% of patients were not weighed. Dysnatraemic patients had a higher hospital mortality rate than those who did not develop dysnatraemia (12.7 vs. 2.3%, P < 0.001).
Conclusions
Four percent of surgical inpatients developed dysnatraemias, which were associated with increased mortality. Fluid balance documentation was suboptimal and daily weights were not measured routinely, even in patients with severe electrolyte derangements.
Similar content being viewed by others

References
Sterns RH, Silver SM (2003) Salt and water: read the package insert. QJM 96:549–552
Awad S, Allison SP, Lobo DN (2008) Fluid and electrolyte balance: the impact of goal directed teaching. Clin Nutr 27:473–478
Walsh SR, Cook EJ, Bentley R et al (2008) Perioperative fluid management: prospective audit. Int J Clin Pract 62:492–497
Walsh SR, Walsh CJ (2005) Intravenous fluid-associated morbidity in postoperative patients. Ann R Coll Surg Engl 87:126–130
Lobo DN, Dube MG, Neal KR et al (2001) Problems with solutions: drowning in the brine of an inadequate knowledge base. Clin Nutr 20:125–130
Lobo DN, Dube MG, Neal KR (2002) Peri-operative fluid and electrolyte management: a survey of consultant surgeons in the UK. Ann R Coll Surg Engl 84:156–160
Lobo DN (2004) Sir David Cuthbertson medal lecture. Fluid, electrolytes and nutrition: physiological and clinical aspects. Proc Nutr Soc 63:453–466
Callum KG, Gray AJG, Hoile RW et al (1999) Extremes of age: the 1999 report of the national confidential enquiry into perioperative deaths. National Confidential Enquiry into Perioperative Deaths, London
Lowell JA, Schifferdecker C, Driscoll DF et al (1990) Postoperative fluid overload: not a benign problem. Crit Care Med 18:728–733
Palevsky PM, Bhagrath R, Greenberg A (1996) Hypernatremia in hospitalized patients. Ann Intern Med 124:197–203
Polderman KH, Schreuder WO, van Schijndel R et al (1999) Hypernatremia in the intensive care unit: an indicator of quality of care? Crit Care Med 27:1105–1108
Sterns RH (1999) Hypernatremia in the intensive care unit: instant quality-just add water. Crit Care Med 27:1041–1042
Powell-Tuck J, Gosling P, Lobo DN et al. (2008) British consensus guidelines on intravenous fluid therapy for adult surgical patients—GIFTASUP. Available at http://www.ics.ac.uk/downloads/2008112340_GIFTASUP%20FINAL_31-10-08.pdf. Accessed 12 July 2009
Steele A, Gowrishankar M, Abrahamson S et al (1997) Postoperative hyponatremia despite near-isotonic saline infusion: a phenomenon of desalination. Ann Intern Med 126:20–25
Caramelo C, Tejedor A, Criado C et al (2008) Fluid therapy in surgical patients: composition and influences on the internal milieu. Nefrologia 28:37–42
Kumar S, Berl T (1998) Sodium. Lancet 352:220–228
Veech RL (1986) The toxic impact of parenteral solutions on the metabolism of cells: a hypothesis for physiological parenteral therapy. Am J Clin Nutr 44:519–551
Reid F, Lobo DN, Williams RN et al (2003) (Ab)normal saline and physiological Hartmann’s solution: a randomized double-blind crossover study. Clin Sci (Lond) 104:17–24
Awad S, Allison SP, Lobo DN (2008) The history of 0.9% saline. Clin Nutr 27:179–188
Streeten DH, Ward-McQuaid JN (1952) Relation of electrolyte changes and adrenocortical activity to paralytic ileus. Br Med J 2:587–592
Halperin ML, Kamel KS (1998) Potassium. Lancet 352:135–140
Batra GS, Molyneux J, Scott NA (2001) Colorectal patients and cardiac arrhythmias detected on the surgical high dependency unit. Ann R Coll Surg Engl 83:174–176
Wise LC, Mersch J, Racioppi J et al (2000) Evaluating the reliability and utility of cumulative intake and output. J Nurs Care Qual 14:37–42
Lindner G, Funk GC, Schwarz C et al (2007) Hypernatremia in the critically ill is an independent risk factor for mortality. Am J Kidney Dis 50:952–957
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Herrod, P.J.J., Awad, S., Redfern, A. et al. Hypo- and Hypernatraemia in Surgical Patients: Is There Room for Improvement?. World J Surg 34, 495–499 (2010). https://doi.org/10.1007/s00268-009-0374-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-009-0374-y