
Abstract
Background
The recent development and spread of ultrasonography and ultrasonography-guided fine needle aspiration biopsy (FNAB) has facilitated the detection of small papillary microcarcinomas of the thyroid measuring 1 cm or less (PMC). The marked difference in prevalence between clinical thyroid carcinoma and PMC detected on mass screening prompted us to observe PMC unless the lesion shows unfavorable features, such as location adjacent to the trachea or on the dorsal surface of the thyroid possibly invading the recurrent laryngeal nerve, clinically apparent nodal metastasis, or high-grade malignancy on FNAB findings. In the present study we report comparison of the outcomes of 340 patients with PMC who underwent observation and the prognosis of 1,055 patients who underwent immediate surgery without observation.
Methods
Between 1993 and 2004, 340 patients underwent observation and 1,055 underwent surgical treatment without observation. These 1,395 patients were enrolled in the present study. Observation periods ranged from 18 to 187 months (average 74 months).
Results
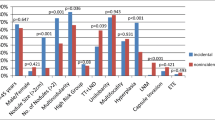
The proportions of patients whose PMC showed enlargement by 3 mm or more were 6.4 and 15.9% on 5-year and 10-year follow-up, respectively. Novel nodal metastasis was detected in 1.4% at 5 years and 3.4% at 10 years. There were no factors related to patient background or clinical features linked to either tumor enlargement or the novel appearance of nodal metastasis. After observation 109 of the 340 patients underwent surgical treatment for various reasons, and none of those patients showed carcinoma recurrence. In patients who underwent immediate surgical treatment, clinically apparent lateral node metastasis (N1b) and male gender were recognized as independent prognostic factors of disease-free survival.
Conclusions
Papillary microcarcinomas that are not associated with unfavorable features can be candidates for observation regardless of patient background and clinical features. If there are subsequent signs of progression, such as tumor enlargement and novel nodal metastasis, it would not be too late to perform surgical treatment. Even though the primary tumor is small, careful surgical treatment including therapeutic modified neck dissection is necessary for N1b PMC patients.





Similar content being viewed by others


References
Sobin LH, Wittekind CH (eds) (2002) UICC: TNM classification of malignant tumors, 6th edn. Wiley-Liss, New York
Ito Y, Tomoda C, Uruno T et al (2005) Ultrasound-detectable and anatomopathologically detectable node metastasis in the lateral compartment as indicators of worse relapse-free survival in patients with papillary thyroid carcinoma. World J Surg 29:917–920
Ito Y, Tomoda C, Uruno T et al (2006) Prognostic significance of extrathyroid extension of papillary thyroid carcinoma: massive but not minimal extension affects the relapse-free survival. World J Surg 30:780–786
Ito Y, Miyauchi A, Jikuzono T et al (2007) Risk factors contributing to a poor prognosis of papillary thyroid carcinoma; validity of UICC/AJCC TNM classification and stage grouping. World J Surg 31:838–848
Yokozawa T, Miyauchi A, Kuma K et al (1995) Accurate and simple method of diagnosing thyroid nodules by the modified technique of ultrasound-guided fine needle aspiration biopsy. Thyroid 5:141–145
Takebe K, Date M, Yamamoto Y et al (1994) Mass screening for thyroid cancer with ultrasonography. KARKINOS 7:309–317 (in Japanese)
Harach HR, Franssila KO, Wasenius VM (1985) Occult papillary carcinoma of the thyroid: a “normal” finding in Finland. A systematic autopsy study. Cancer 56:531–538
Fukunaga FH, Yatani R (1975) Geographic pathology of occult thyroid carcinomas. Cancer 36:1095–1099
Samson RJ (1977) Prevalence and significant of occult thyroid cancer. In: DeGroot LJ (ed) Radiation-associated thyroid carcinoma. Grune & Stratton, New York, pp 137–153
Thorvaldsson SE, Tulinius H, Bjornsson J et al (1992) Latent thyroid carcinoma in Iceland at autopsy. Pathol Res Pract 188:747–750
Iida F, Sugenoya A, Muramatsu A (1991) Clinical and pathologic properties of small differentiated carcinomas of the thyroid gland. World J Surg 15:511–515
Hay ID, Grant CS, van Heerden JA et al (1992) Papillary thyroid microcarcinoma: a study of 535 cases observed in a 50-year period. Surgery 112:1139–1147
Rodriguez JM, Moreno A, Parrila P et al (1997) Papillary thyroid microcarcinoma: clinical study and prognosis. Eur J Surg 163:255–259
Lin KD, Lin JD, Huang MJ et al (1997) Clinical presentations and predictive variables of thyroid microcarcinoma with distant metastasis. Int Surg 82:378–381
Rassael H, Thompson LDR, Heffess CS (1998) A rationale for conservative management of microscopic papillary carcinoma of the thyroid gland: a clinicopathological correlation of 90 cases. Eur Arch Otorhinolaryngol 255:462–467
Sugitani I, Fumimoto Y (1999) Symptomatic versus asymptomatic papillary thyroid microcarcinoma: a retrospective analysis of surgical outcome and prognostic factors. Endocine J 46:209–216
Falvo L, D’Ercole C, Sorrenti S et al (2003) Papillary microcarcinoma of the thyroid gland: analysis of prognostic factors including histological subtype. Eur J Surg 168:28–32
Wada N, Duh QY, Sugino K et al (2003) Lymph node metastasis from 259 papillary thyroid microcarcinomas. Ann Surg 237:399–407
Chow SM, Law SCK, Chan JK (2003) Papillary microcarcinoma of the thyroid—prognostic significance of lymph node metastasis and multifocally. Cancer 98:31–40
Ito Y, Tomoda C, Uruno T et al (2004) Papillary microcarcinoma of the thyroid: how should it be treated? World J Surg 28:1115–1121
Ito Y, Uruno R, Nakano K et al (2003) An observation trial without surgical treatment in patients with papillary microcarcinoma of the thyroid. Thyroid 13:381–388
Ito Y, Miyauchi A (2007) A therapeutic strategy for incidentally detected papillary microcarcinoma of the thyroid. Nature Clin Pract Endocrinol Metab 3:240–248
Ito Y, Miyauchi A (2007) Appropriate treatment for asymptomatic papillary microcarcinoma of the thyroid. Exp Opin Pharmacother 8:3205–3215
Grossman RF, Tu SH, Duh QY (1995) Familial nonmedullary thyroid cancer. An emerging entity that warrants aggressive treatment. Arch Surg 130:892–897
Uruno T, Miyauchi A, Shimizu K et al (2005) Usefulness of thyroglobulin measurement in fine-needle aspiration biopsy specimens for diagnosing cervical lymph node metastasis in patients with papillary thyroid cancer. World J Surg 29:483–485
Uchino S, Noguchi S, Kawamoto H et al (2002) Familial nonmedullary thyroid carcinoma characterized by multifocality and a high recurrence rate in a large study population. World J Surg 26:897–902
Ito Y, Kakudo K, Hirokawa M et al (2009) Biological behavior and prognosis of familial papillary thyroid carcinoma. Surgery 145:100–105
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ito, Y., Miyauchi, A., Inoue, H. et al. An Observational Trial for Papillary Thyroid Microcarcinoma in Japanese Patients. World J Surg 34, 28–35 (2010). https://doi.org/10.1007/s00268-009-0303-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-009-0303-0