
Abstract
Background
Gastric cancer with esophageal invasion (GCE) is a disease of poor prognosis, and issues pertaining to surgical treatment still remain unresolved. Particularly problematic areas in GCE cases include the need for lower mediastinal lymph node (MSLN) dissection, the most effective surgical approach, and the optimal extent of the esophageal resection. In this study, we evaluate the characteristics of GCE and investigate aspects of surgical treatment.
Methods
Sixty-five patients with GCE were surgically treated in our department from 1990 to 2007. Fifty-two patients with M0 were evaluated for clinicopathological factors, disease recurrence pattern, and prognosis, and 47 patients with R0 resection were evaluated for operative factors.
Results
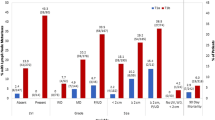
Patients with MSLN metastasis had significantly poor prognosis. The survival rate significantly differed among patients depending on T-factor, LN metastasis, MSLN metastasis, and lymphatic vessel invasion, but operative factors were not significant prognostic factors. Multivariate analysis indicated that T-factor and MSLN metastasis were independent prognostic factors. The peritoneum was the site of the highest recurrence rate (26.9%), followed by the liver (9.6%). Peritoneal recurrence correlated with T-factor and lymphatic vessel invasion and liver recurrence correlated with MSLN metastasis.
Conclusions
It seems that radical MSLN dissection and extended esophageal resection by thoracotomy have little therapeutic purpose for Siewert Types II or III tumors in GCE if the length of esophageal resection is within 6 cm. Patients with GCE have a poorer prognosis than those with common gastric cancer, and early detection and multimodal treatments for distant metastases are vital for ameliorating clinical outcome in patients with GCE.



Similar content being viewed by others


References
Blot WJ, Devesa SS, Kneller RW, Fraumeni JF Jr (1991) Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA 265:1287–1289
Powell J, McConkey CC (1992) The rising trend in oesophageal adenocarcinoma and gastric cardia. Eur J Cancer Prev 1:265–269
Pera M, Cameron AJ, Trastek VF et al (1993) Increasing incidence of adenocarcinoma of the esophagus and esophagogastric junction. Gastroenterology 104:510–513
Moriwaki Y, Kunisaki C, Kobayashi S et al (2003) Progressive improvement of prognosis for patients with gastric cancer (dynamic stage grouping) with increasing survival interval from initial staging: how much longer can a given survivor expect to live? Surgery 133:135–140
Maehara Y, Kakeji Y, Oda S et al (2000) Time trends of surgical treatment and the prognosis for Japanese patients with gastric cancer. Br J Cancer 83:986–991
Itoh H, Oohata Y, Nakamura K et al (1989) Complete 10-year postgastrectomy follow-up of early gastric cancer. Am J Surg 158:14–16
Abe S, Ogawa Y, Nagasue N et al (1984) Early gastric cancer: results in a general hospital in Japan. World J Surg 8:308–314
Ito H, Clancy TE, Osteen RT et al (2004) Adenocarcinoma of the gastric cardia: what is the optimal surgical approach? J Am Coll Surg 199:880–886
Rudiger Siewert J, Feith M, Werner M, Stein HJ (2000) Adenocarcinoma of the esophagogastric junction: results of surgical therapy based on anatomical/topographic classification in 1,002 consecutive patients. Ann Surg 232:353–361
Nishi M, Nomura H, Kajisa T et al (1978) Surgical problem of carcinoma in the esophagogastric junction. Stomach and Intestine 13:1497–1507
Siewert JR, Stein HJ (1998) Classification of adenocarcinoma of the oesophagogastric junction. Br J Surg 85:1457–1459
Kawaura Y, Mori Y, Nakajima H, Iwa T (1988) Total gastrectomy with left oblique abdominothoracic approach for gastric cancer involving the esophagus. Arch Surg 123:514–518
Kodama I, Kofuji K, Yano S et al (1998) Lymph node metastasis and lymphadenectomy for carcinoma in the gastric cardia: clinical experience. Int Surg 83:205–209
Maruyama K, Sasako M, Kinoshita T et al (1996) Surgical treatment for gastric cancer: the Japanese approach. Semin Oncol 23:360–368
Yonemura Y, Tsugawa K, Fonseca L et al (1995) Lymph node metastasis and surgical management of gastric cancer invading the esophagus. Hepatogastroenterology 42:37–42
Japanese Gastric Cancer Association (1998) Japanese classification of gastric carcinoma, 2nd English edn. Gastric Cancer 1:10–24
Sobin LH, Fleming ID (1997) TNM classification of malignant tumors, 5th edn, Union Internationale Contre le Cancer and the American Joint Committee on Cancer. Cancer 80:1803–1804
Husemann B (1989) Cardia carcinoma considered as a distinct clinical entity. Br J Surg 76:136–139
Bozzetti F, Bignami P, Bertario L et al (2000) Surgical treatment of gastric cancer invading the oesophagus. Eur J Surg Oncol 26:810–814
Wayman J, Dresner SM, Raimes SA, Griffin SM (1999) Transhiatal approach to total gastrectomy for adenocarcinoma of the gastric cardia. Br J Surg 86:536–540
Nunobe S, Ohyama S, Sonoo H et al (2008) Benefit of mediastinal and para-aortic lymph-node dissection for advanced gastric cancer with esophageal invasion. J Surg Oncol 97:392–395
Moon MR, Schulte WJ, Haasler GB, Condon RE (1992) Transhiatal and transthoracic esophagectomy for adenocarcinoma of the esophagus. Arch Surg 127:951–955
Griffin SM, Chung SC, Woods SD, Li AK (1990) Adenocarcinoma of the cardia: treatment by thoracoabdominal R3 radical gastrectomy. Br J Surg 77:937–939
Griffith JL, Davis JT (1980) A 20-year experience with surgical management of carcinoma of the esophagus and gastric cardia. J Thorac Cardiovasc Surg 79:447–452
Millikan KW, Silverstein J, Hart V et al (1995) A 15-year review of esophagectomy for carcinoma of the esophagus and cardia. Arch Surg 130:617–624
Finley RJ, Grace M, Duff JH (1985) Esophagogastrectomy without thoracotomy for carcinoma of the cardia and lower part of the esophagus. Surg Gynecol Obstet 160:49–56
Tanigawa N, Shimomatsuya T, Horiuchi T et al (1993) En bloc resection for cancer of the gastric cardia without thoracotomy. J Surg Oncol 54:23–28
Sasako M, Sano T, Yamamoto S et al (2006) Left thoracoabdominal approach versus abdominal-transhiatal approach for gastric cancer of the cardia or subcardia: a randomised controlled trial. Lancet Oncol 7:644–651
Mori A, Mori S (1985) Contraction rate of esophageal specimen. Jpn J Gastroenterol Surg 18:2270–2272
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wakatsuki, K., Takayama, T., Ueno, M. et al. Characteristics of Gastric Cancer with Esophageal Invasion and Aspects of Surgical Treatment. World J Surg 33, 1446–1453 (2009). https://doi.org/10.1007/s00268-009-0053-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-009-0053-z