
Abstract
Purpose
Resection line infiltration (RLI) after surgical treatment represents an unfavorable prognostic factor in advanced gastric cancer. We performed a retrospective analysis of 89 patients with resection line involvement who did not undergo reoperation.
Methods
On behalf of the Italian Research Group for Gastric Cancer, we present the characteristics and outcome of 89 patients who were submitted to surgical resection for gastric cancer from 1988 to 2001 and did not undergo reoperation because of disease extension or associated pathologies.
Results
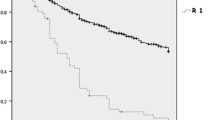
RLI was significantly higher in patients with T4 tumors and diffuse histological type. Anastomotic leakages were observed in 4.8% of infiltrated esophageal resection margins, whereas 1.9% of infiltrated duodenal resection lines showed duodenal fistulas. Five-year overall survival of patients with RLI was 29%. Prognosis was not affected by RLI in early forms (100% 5-year survival); however, 5-year survival in T2 and T3 stages was significantly lower with respect to the same stages without residual tumor. The influence of RLI on prognosis was confirmed in N0 as well as in N1 and N2 patients. RLI also was an independent prognostic at multivariate analysis (odds ratio = 1.5; 95% confidence interval, 1.08–2.08; P = 0.0144).
Conclusions
RLI significantly affects long-term survival of advanced gastric cancer. The impact on prognosis is independent of lymph node involvement. Patients in good general condition for whom radical surgery is possible should be considered for reoperation.

Similar content being viewed by others


References
Songun I, Bonekamp JJ, Hermans J et al (1996) Prognostic value of resection line involvement in patients undergoing curative resection for gastric cancer. Eur J Cancer 32A:433–437
Hallissey MT, Jewkes AJ, Dunn JA et al (1993) Resection-line involvement in gastric cancer: a continuing problem. Br J Surg 80:1418–1420
Nakamura K, Ueyama T, Yao T et al (1992) Pathology and prognosis of gastric carcinoma. Findings in 10,000 patients who underwent primary gastrectomy. Cancer 70:1030–1037
Morgagni P, Garcea D, Marrelli D et al (2006) Does resection line involvement affect prognosis in early gastric cancer patients? An Italian multicentric study. World J Surg 30:585–589
Papachristou DN, Agnanti N, D’Agostino H et al (1980) Histologically positive esophageal margin in the treatment of gastric cancer. Am J Surg 139:711–713
Japanese Research Society for Gastric Cancer (1995) Japanese classification of gastric carcinoma. Japanese Research Society for Gastric Cancer. Kanehara, Tokyo, pp 15–16
Lauren P (1965) The two histological main types of gastric carcinoma: diffuse and so-called intestinal type carcinoma. An attempt at a histo-clinical classification. Acta Pathol Microbiol Scand 64:31–49
Sobin LH, Wittekind C (1997) TNM classification of malignant tumors, 5th edn. Wiley, New York
Roviello F, Marrelli D, Morgagni P et al (2002) Survival benefit of extended D2 lymphadenectomy in gastric cancer with involvement of second level lymph nodes: a longitudinal multicenter study. Ann Surg Oncol 9:894–900
Kaplan EL, Meier P (1958) Non parametric estimation from incomplete observation. J Am Stat Assoc 53:457–481
Mantel N (1966) Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother Rep 50:163–170
Cox DR (1972) Regression models and life tables. J Royal Stat Soc 34:187–220
Institute Inc SAS (1989) SAS/STAT user’s guide version 8.02, vol 1. SAS Institute, Cary, NC
Tsujitani S, Okuyama T, Orita H et al (1995) Margins of resection of the esophagus for gastric cancer with esophageal invasion. Hepatogastroenterology 42:873–877
Yokota T, Kunii Y, Teshima S et al (1999) Clinicopathologic prognostic features in patients with gastric cancer associated with esophageal or duodenal invasion. Ups J Med Sci 104:217–230
Bozzetti F, Bonfanti G, Bufalino R et al (1982) Adequacy of margins of resection in gastrectomy for cancer. Ann Surg 196:685–690
Kakeji Y, Tsujitani S, Baba H et al (1991) Clinicopathologic features and prognostic significance of duodenal invasion in patients with distal gastric carcinoma. Cancer 68:380–384
Fujimoto S, Takahashi M, Mutou T et al (1997) Clinicopathologic characteristics of gastric cancer patients with cancer infiltration at surgical margin at gastrectomy. Anticancer Res 17:689–694
Keighley MR, Moore J, Lee JR et al (1981) Perioperative frozen section and cytology to assess proximal invasion in gastro-esophageal carcinoma. Br J Surg 68:73–74
Chan WH, Wong WK, Khin LW et al (2000) Significance of a positive oesophageal margin in stomach cancer. Aust N Z J Surg 70:700–703
Sano T, Mudan SS (1999) No advantage of reoperation for positive resection margin in node positive gastric cancer patients? Jpn J Clin Oncol 29:283–284
Cascinu S, Giordani P, Catalano V et al (1999) Resection-line involvement in gastric cancer patients undergoing curative resections: implications for clinical management. Jpn J Clin Oncol 29:291–293
Kim SH, Karpeh MS, Klimstra DS et al (1999) Effect of microscopic resection line disease on gastric cancer survival. J Gastrointest Surg 3:24–33
Nagano H, Ohyama S, Fukunaga T et al (2005) Indications for gastrectomy after incomplete EMR for early gastric cancer. Gastric Cancer 8:149–154
Marrelli D, De Stefano A, de Manzoni G et al (2005) Prediction of recurrence after radical surgery for gastric cancer: a scoring system obtained from a prospective multicentric study. Ann Surg 241:247–255
Roviello F, Marrelli D, de Manzoni G et al (2003) Prospective study of peritoneal recurrence after curative surgery for gastric cancer. Br J Surg 90:1113–1119
Saka M, Mudan SS, Katai H et al (2005) Pancreaticoduodenectomy for advanced gastric cancer. Gastric Cancer 8:1–5
Acknowledgments
The authors thank Gráinne Tierney for assistance.
Author information
Authors and Affiliations
Corresponding author
Additional information
All the authors are for the Italian Research Group for Gastric Cancer (I.R.G.G.C.).
Rights and permissions
About this article
Cite this article
Morgagni, P., Garcea, D., Marrelli, D. et al. Resection Line Involvement After Gastric Cancer Surgery: Clinical Outcome in Nonsurgically Retreated Patients. World J Surg 32, 2661–2667 (2008). https://doi.org/10.1007/s00268-008-9747-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-008-9747-x