
Abstract
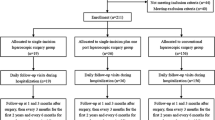
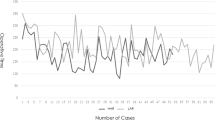
This study aimed to compare medial-to-lateral versus lateral-to-medial laparoscopic dissection sequences for resecting rectosigmoid cancers. We hypothesized that the medial-to-lateral approach was a more efficient procedure and with potentially better oncologic results. Between January 1997 and June 1999, a total of 67 patients of rectosigmoid cancer treated by one surgeon using the laparoscopic approach were recruited for this prospective, randomized, double-blind clinical trial. Using the blocked randomization method, 36 patients were allocated to a medial-to-lateral (M) group and the other 31 to a lateral-to-medial (L) group; the groups were well matched in age, gender, symptoms, body mass index, American Society of Anesthesiology (ASA) class, tumor location, tumor distance above the anal verge, tumor gross morphology, TNM stage of the tumor, and accuracy of preoperative TNM staging (p > 0.05). All patients were followed up until June 2001. We found that the M group had a significantly shorter operating time and lower overall costs than the L group (p < 0.05). There was no significant difference between these two groups in terms of intraoperative complications, conversion rate, postoperative ileus, hospitalization, postoperative pain, postoperative complications, wound length, or disability (p > 0.05). The postoperative proinflammatory response, evaluated by the C-reactive protein level and the erythrocyte sedimentation rate, was significantly lower in the M group (p < 0.05). There was no significant difference between these two groups regarding postoperative immunosuppression, as evaluated by the alterations of total lymphocyte counts and the CD4+/CD8+ ratio (p > 0.05). The extent of dissection of these two dissection approaches was similar, as the harvested lymph nodes were equivalent (p > 0.05). During the whole follow-up period (median 32 months, range 24–54 months), the tumor recurrence rate was similar for these two groups of patients (5.6% in the M group vs. 6.5% in the L group; p > 0.05). These findings indicated that the medial-to-lateral approach was quicker, less expensive and possibly less invasive; moreover, it gave oncologic results similar to those achieved with the traditional lateral-to-medial dissection sequence. We thus concluded that the medial-to-lateral dissection sequence may currently be the most appropriate procedure for laparoscopic resection of rectosigmoid cancers.
Similar content being viewed by others

Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Liang, JT., Lai, HS., Huang, KC. et al. Comparison of Medial-to-lateral versus Traditional Lateral-to-medial Laparoscopic Dissection Sequences for Resection of Rectosigmoid Cancers: Randomized Controlled Clinical Trial. World J. Surg. 27, 190–196 (2003). https://doi.org/10.1007/s00268-002-6437-y
Issue Date:
DOI: https://doi.org/10.1007/s00268-002-6437-y