
Abstract
Purpose
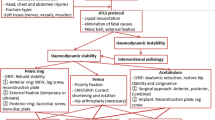
Floating hip fractures are severe and rare injuries with high complication rate and lack of standard management. The purpose of this retrospective study was to review the outcomes of a case series of polytraumatized patients with floating hip injuries, in order to describe the relationship between complication rate and floating hip injury type, the pathomechanism of injury, and the surgical treatment strategy.
Methods
Forty-five patients with floating hip injuries were analyzed. Complication rate, mechanism of injury, and surgical strategy (damage control orthopedics, stages of internal fixation) were recorded. Fractures were classified using the Mueller system for floating hips and AO/OTA system for the other fractures.
Results
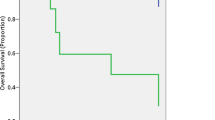
Of the 45 patients with floating hip injuries, 23 (51.1%) developed complications. The results revealed that the complication rate was associated with the instability and type of the pelvic or acetabular fracture (61-C AO/OTA pelvic fracture [73.3%; p = 0.04], 62-B AO/OTA acetabular fracture [88.8%; p = 0.03]). Vertical shear (VS) pelvic fractures were related to middle-distal femoral fractures and lateral compression/anteroposterior compression (LC/APC) pelvic lesions were associated to proximal femoral fractures (p = 0.012).
Conclusions
Complications were associated with the severity and instability of the pelvic and acetabular type of fractures. The pathomechanism causing Mueller type B and C floating hip injuries was illustrated. A two-stage “femur first” surgical approach was the preferred one for definite internal fixation of fractures.



Similar content being viewed by others

Data availability
Data can be made available upon request.
Change history
29 November 2021
A Correction to this paper has been published: https://doi.org/10.1007/s00264-021-05270-4
References
Simpson NS, Jupiter JB (1995) Complex fracture patterns of the upper extremity. Clin Orthop Relat Res 318:43–53
Mohamed SO, Ju W, Qin Y, Qi B (2019) The term “floating” used in traumatic orthopedics. Medicine (Baltimore) 98(7), e14497
Liebergall M, Lowe J, Whitelaw GP, Wetzler MJ, Segal D (1992) The floating hip. Ipsilateral pelvic and femoral fractures. Bone Joint Surg Br 74:93–100
Bishop JA, Cross WW 3rd, Krieg JC, Chip Routt ML, Jr, (2013) Antegrade femoral nailing in acetabular fractures requiring a Kocher-Langenbeck approach. Orthopedics 36(9):e1159–e1164
Cannada LK, Hire JM, Boyer PJ, Israel H, Mir H, Halvorson J, Della Rocca GJ, Ming B, Mullis B, Deshpande C (2017) Treatment and complications of patients with ipsilateral acetabular and femur fractures: a multicenter retrospective analysis. J Orthop Trauma 31(12):650–656
Wei L, Sun JY, Wang Y, Yang X (2011) Surgical treatment and prognosis of acetabular fractures associated with ipsilateral femoral neck fractures. Orthopedics 34(5):348
Muller EJ, Siebenrock K, Ekkernkamp A, Ganz R, Muhr G (1999) Ipsilateral fractures of the pelvis and the femur–floating hip? A retrospective analysis of 42 cases. Arch Orthop Trauma Surg 119:179–182
Burd TA, Hughes MS, Anglen JO (2008) The floating hip: complications and outcomes. J Trauma 64:442–448
Zamora-Navas P, Guerado E (2010) Vascular complications in floating hip. Hip Int 20(Suppl 7):S11–S18
Liebergall M, Mosheiff R, Safran O, Peyser A, Segal D (2002) The floating hip injury: patterns of injury 33:717–722
Kregor PJ, Templeman D (2002) Associated injuries complicating the management of acetabular fractures: review and case studies. Orthop Clin North Am 33:73–95
Meinberg EG et al (2018) Fracture and dislocation classification compendium. J Orthop Trauma 32(Suppl 1):S1–S170
Young JW, Burgess AR, Brumback RJ, Poka A (1986) Pelvic fractures: value of plain radiography in early assessment and management. Radiology 160(2):445–451
Pipkin G (1957) Treatment of grade IV fracture dislocation of the hip. J Bone Joint Surg Am 39:1027–1042
Kates B (2017) Principles of orthopedic infection management. Thieme
Anderson, Bruce Browner Jesse Jupiter, Christian Krettek Paul (2014) Skeletal trauma: basic science, management, and reconstruction, 2-Volume Set. Elsevier
Zamora-Navas P, Estades-Rubio FJ, Cano JR, Guerado E (2017) Floating hip and associated injuries. Injury 48(Suppl 6):S75–S80
Suzuki T, ShindoM SK (2006) The floating hip injury: which should we fix first? Eur J Orthop Surg Traumatol 16(214):8
Manson TT, Nascone JW, O’Toole RV (2010) Traction vertical shear pelvic ring fracture: a marker for severe arterial injury? A case report J Orthop Trauma 24(10):e90–e94
Cech A, Rieussec C, Kerschbaumer G, Seurat O, Corbet C, Vibert B, Tronc C, Ruatti S, Bouzat P, Tonetti J, Boudissa M. (2021) Complications and outcomes in 69 consecutive patients with floating hip. Orthop Traumatol Surg Res. doi: https://doi.org/10.1016/j.otsr.2021.102998. Epub ahead of print.
Author information
Authors and Affiliations
Contributions
MB and DC initiated the study and set up the design. MB collected and analyzed data. MB wrote the manuscript. FR, PC, and DC revised every version. All authors reviewed the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
All procedures performed were in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent to participate
Not applicable to this retrospective study.
Consent for publication
The authors and institutions have consented to publication.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original version of this article was revised. The names of all authors are inverted.
Rights and permissions
About this article

Cite this article
Brioschi, M., Randelli, F., Capitani, P. et al. Floating hip in polytraumatized patients: complications, mechanism of injury, and surgical strategy. International Orthopaedics (SICOT) 46, 361–368 (2022). https://doi.org/10.1007/s00264-021-05262-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-021-05262-4