
Abstract
Purpose
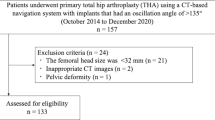
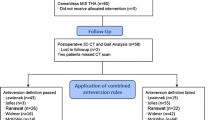
In this prospective study of 135 patients undergoing cementless total hip arthroplasty (THA) we asked whether six current definitions of combined anteversion prevent impingement and increase postoperative patient individual impingement-free range-of-motion (ROM).
Methods
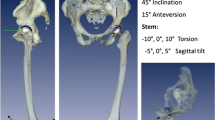
Implant position was measured by an independent, external institute on 3D-CT performed six weeks post-operatively. Post-operative ROM was calculated using a CT-based algorithm detecting osseous and/or prosthetic impingement by virtual hip movement. Additionally, clinical ROM was evaluated pre-operatively and one-year post-operatively by a blinded observer.
Results
Combined component position of cup and stem according to the definitions of Ranawat, Widmer, Dorr, Hisatome and Yoshimine inhibited prosthetic impingement in over 90 %, while combined osseous and prosthetic impingement still occurred in over 40 % of the cases. The recommendations by Jolles, Widmer, Dorr, Yoshimine and Hisatome enabled higher flexion (p ≤ 0.001) and internal rotation (p ≤ 0.006). Clinically, anteversion rules of Widmer and Yoshimine provided one-year post-operatively statistically but not clinically relevant higher internal rotation (p ≤0.034).
Conclusion
Standard rules of combined anteversion detect prosthetic but fail to prevent combined osseous and prosthetic impingement in THA. Future models will have to account for the patient-individual anatomic situation to ensure impingement-free ROM.





Similar content being viewed by others
References
Widmer KH (2004) A simplified method to determine acetabular cup anteversion from plain radiographs. J Arthroplasty 19:387–390
Dorr LD, Malik A, Dastane M, Wan Z (2009) Combined anteversion technique for total hip arthroplasty. Clin Orthop Relat Res 467:119–127. doi:10.1007/s11999-008-0598-4
Malik A, Maheshwari A, Dorr LD (2007) Impingement with total hip replacement. J Bone Joint Surg Am 89:1832–1842. doi:10.2106/JBJS.F.01313
Miki H, Yamanashi W, Nishii T, Sato Y, Yoshikawa H, Sugano N (2007) Anatomic hip range of motion after implantation during total hip arthroplasty as measured by a navigation system. J Arthroplasty 22:946–952. doi:10.1016/j.arth.2007.02.004
McKibbin B (1970) Anatomical factors in the stability of the hip joint in the newborn. J Bone Joint Surg (Br) 52:148–159
Jolles BM, Zangger P, Leyvraz PF (2002) Factors predisposing to dislocation after primary total hip arthroplasty: a multivariate analysis. J Arthroplasty 17:282–288
Widmer KH, Zurfluh B (2004) Compliant positioning of total hip components for optimal range of motion. J Orthop Res 22:815–821. doi:10.1016/j.orthres.2003.11.001
Hisatome T, Doi H (2011) Theoretically optimum position of the prosthesis in total hip arthroplasty to fulfill the severe range of motion criteria due to neck impingement. J Orthop Sci 16:229–237. doi:10.1007/s00776-011-0039-1
Yoshimine F (2006) The safe-zones for combined cup and neck anteversions that fulfill the essential range of motion and their optimum combination in total hip replacements. J Biomech 39:1315–1323. doi:10.1016/j.jbiomech.2005.03.008
Ranawat CS, Maynard MJ (1991) Modern technique of cemented total hip arthroplasty. Tech Orthop 6:17–2510. doi:10.1054/arth.2001.24442
Parratte S, Pagnano MW, Coleman-Wood K, Kaufman KR, Berry DJ (2009) The 2008 Frank Stinchfield award: variation in postoperative pelvic tilt may confound the accuracy of hip navigation systems. Clin Orthop Relat Res 467:43–49. doi:10.1007/s11999-008-0521-z
Weber M, Weber T, Woerner M, Craiovan B, Worlicek M, Winkler S, Grifka J, Renkawitz T (2015) The impact of standard combined anteversion definitions on gait and clinical outcome within one year after total hip arthroplasty. Int Orthop 39(12):2323–33. doi:10.1007/s00264-015-2777-8
Wan Z, Malik A, Jaramaz B, Chao L, Dorr LD (2009) Imaging and navigation measurement of acetabular component position in THA. Clin Orthop Relat Res 467:32–42. doi:10.1007/s11999-008-0597-5
Renkawitz T, Haimerl M, Dohmen L, Gneiting S, Wegner M, Ehret N, Buchele C, Schubert M, Lechler P, Woerner M, Sendtner E, Schuster T, Ulm K, Springorum R, Grifka J (2011) Minimally invasive computer-navigated total hip arthroplasty, following the concept of femur first and combined anteversion: design of a blinded randomized controlled trial. BMC Musculoskelet Disord 12:192. doi:10.1186/1471-2474-12-192
Pijls BG, Dekkers OM, Middeldorp S, Valstar ER, van der Heide HJ, Van der Linden-Van der Zwaag HM, Nelissen RG (2011) AQUILA: assessment of quality in lower limb arthroplasty. An expert Delphi consensus for total knee and total hip arthroplasty. BMC Musculoskelet Disord 12:173. doi:10.1186/1471-2474-12-173
Michel MC, Witschger P (2007) MicroHip: a minimally invasive procedure for total hip replacement surgery using a modified Smith-Peterson approach. Ortop Traumatol Rehabil 9:46–51
Renkawitz T, Haimerl M, Dohmen L, Woerner M, Springorum HR, Sendtner E, Heers G, Weber M, Grifka J (2012) Development and evaluation of an image-free computer-assisted impingement detection technique for total hip arthroplasty. Proc Inst Mech Eng H 226:911–918. doi:10.1177/0954411912460815
Renkawitz T, Weber M, Springorum HR, Sendtner E, Woerner M, Ulm K, Weber T, Grifka J (2015) Impingement-free range of movement, acetabular component cover and early clinical results comparing 'femur-first' navigation and 'conventional' minimally invasive total hip arthroplasty: a randomised controlled trial. Bone Joint J 97-B:890–898. doi:10.1302/0301-620X.97B7.34729
Davis KE, Ritter MA, Berend ME, Meding JB (2007) The importance of range of motion after total hip arthroplasty. Clin Orthop Relat Res 465:180–184. doi:10.1097/BLO.0b013e31815c5a64
Turley GA, Ahmed SM, Williams MA, Griffin DR (2011) Establishing a range of motion boundary for total hip arthroplasty. Proc Inst Mech Eng H 225:769–782
Weber M, Lechler P, von Kunow F, Vollner F, Keshmiri A, Hapfelmeier A, Grifka J, Renkawitz T (2015) The validity of a novel radiological method for measuring femoral stem version on anteroposterior radiographs of the hip after total hip arthroplasty. Bone Joint J 97-B:306–311. doi:10.1302/0301-620X.97B3.34618
Murray DW (1993) The definition and measurement of acetabular orientation. J Bone Joint Surg (Br) 75:228–232
Wines AP, McNicol D (2006) Computed tomography measurement of the accuracy of component version in total hip arthroplasty. J Arthroplasty 21:696–701. doi:10.1016/j.arth.2005.11.008
Hube R, Dienst M, von Roth P (2014) Complications after minimally invasive total hip arthroplasty. Orthopade 43:47–53. doi:10.1007/s00132-013-2123-z
Preininger B, Haschke F, Perka C (2014) Diagnostics and therapy of luxation after total hip arthroplasty. Orthopade 43:54–63. doi:10.1007/s00132-013-2125-x
Park KK, Tsai TY, Dimitriou D, Kwon YM (2016) Three-dimensional in vivo difference between native acetabular version and acetabular component version influences iliopsoas impingement after total hip arthroplasty. Int Orthop. doi:10.1007/s00264-015-3055-5
Tsuda K, Haraguchi K, Koyanagi J, Takahashi S, Sugama R, Fujiwara K (2016) A forty millimetre head significantly improves range of motion compared with a twenty eight millimetre head in total hip arthroplasty using a computed tomography-based navigation system. Int Orthop. doi:10.1007/s00264-015-3095-x
Babisch JW, Layher F, Amiot LP (2008) The rationale for tilt-adjusted acetabular cup navigation. J Bone Joint Surg Am 90:357–365. doi:10.2106/JBJS.F.00628
Renkawitz T, Haimerl M, Dohmen L, Gneiting S, Lechler P, Woerner M, Springorum HR, Weber M, Sussmann P, Sendtner E, Grifka J (2012) The association between Femoral Tilt and impingement-free range-of-motion in total hip arthroplasty. BMC Musculoskelet Disord 13:65. doi:10.1186/1471-2474-13-65
Müller M, Duda G, Perka C, Tohtz S (2016) The sagittal stem alignment and the stem version clearly influence the impingement-free range of motion in total hip arthroplasty: a computer model-based analysis. Int Orthop 40(3):473–80. doi:10.1007/s00264-015-2845-0
Acknowledgments
We thank Dipl-Ing. Mario Schubert for his support in calculations of biomathematical combined anteversion models.
MW and TR originated the idea for the study and led on its design. TR and JG supervised the project. TR, MW, MWOE, BC, MWOR, FV and JG participated in the design of the study. MW, TR, MWOE, BC, MWOR and HS coordinated the experiment and were responsible for data acquisition. HS performed the clinical follow up. MWOR, MWOE, BC and FV were responsible for CT data collection. MW computed implant positions according to the different definitions. MW performed the statistical testing. All authors read and corrected draft versions of the manuscript and approved the final manuscript.
The project upon which this publication is based was funded by the German Federal Ministry of Education and Research (BMBF) under Project Number 01EZ0915.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Weber, M., Woerner, M., Craiovan, B. et al. Current standard rules of combined anteversion prevent prosthetic impingement but ignore osseous contact in total hip arthroplasty. International Orthopaedics (SICOT) 40, 2495–2504 (2016). https://doi.org/10.1007/s00264-016-3171-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-016-3171-x