
Abstract
Purpose
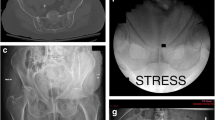
We performed a prospective study to document, by intra-operative manipulation under anaesthesia (MUA) of the pelvic ring, the stability of lateral compression type 1 injuries that were managed in a Level-I Trauma Centre. The documentation of the short-term outcome of the management of these injuries was our secondary aim.
Methods
A total of 63 patients were included in the study. Thirty-five patients (group A) were treated surgically whereas 28 (group B) were managed nonoperatively. Intraoperative rotational instability, evident by more than two centimetres of translation during the manipulation manoeuvre, was combined with a complete sacral fracture in all cases.
Results
A statistically significant difference was present between the length of hospital stay, the time to independent pain-free mobilisation, post-manipulation pain levels and opioid requirements between the two groups, with group A demonstrating significantly decreased values in all these four variables (p < 0.05). There was also a significant difference between the pre- and 72-hour post-manipulation visual analogue scale and analgesic requirements of the group A patients, whereas the patients in group B did not demonstrate such a difference.
Conclusion
LC-1 injuries with a complete posterior sacral injury are inheritably rotationally unstable and patients presenting with these fracture patterns definitely gain benefit from surgical stabilisation.




Similar content being viewed by others


References
Burgess AR, Eastridge BJ, Young JW, Ellison TS, Ellison PS Jr, Poka A, Bathon GH, Brumback RJ (1990) Pelvic ring disruptions: effective classification system and treatment protocols. J Trauma 30(7):848–856
Manson T, O’Toole RV, Whitney A, Duggan B, Sciadini M, Nascone J (2010) Young-Burgess classification of pelvic ring fractures: does it predict mortality, transfusion requirements, and non-orthopaedic injuries? J Orthop Trauma 24(10):603–609. doi:10.1097/BOT.0b013e3181d3cb6b
Mundy AR, Andrich DE (2010) Pelvic fracture-related injuries of the bladder neck and prostate: their nature, cause and management. BJU Int 105(9):1302–1308. doi:10.1111/j.1464-410X.2009.08970.x
Young JW, Burgess AR, Brumback RJ, Poka A (1986) Pelvic fractures: value of plain radiography in early assessment and management. Radiology 160(2):445–451
Khoury A, Kreder H, Skrinskas T, Hardisty M, Tile M, Whyne CM (2008) Lateral compression fracture of the pelvis represents a heterogeneous group of complex 3D patterns of displacement. Injury 39(8):893–902. doi:10.1016/j.injury.2007.09.017
Lefaivre KA, Padalecki JR, Starr AJ (2009) What constitutes a Young and Burgess lateral compression-I (OTA 61-B2) pelvic ring disruption? A description of computed tomography-based fracture anatomy and associated injuries. J Orthop Trauma 23(1):16–21. doi:10.1097/BOT.0b013e31818f8a81
Sagi HC, Coniglione FM, Stanford JH (2011) Examination under anesthetic for occult pelvic ring instability. J Orthop Trauma 25(9):529–536. doi:10.1097/BOT.0b013e31822b02ae
Starr AJ, Nakatani T, Reinert CM, Cederberg K (2008) Superior pubic ramus fractures fixed with percutaneous screws: what predicts fixation failure? J Orthop Trauma 22(2):81–87. doi:10.1097/BOT.0b013e318162ab6e
Denis F, Davis S, Comfort T (1988) Sacral fractures: an important problem. Retrospective analysis of 236 cases. Clin Orthop Relat Res 227:67–81
Manson TT, Nascone JW, Sciadini MF, O’Toole RV (2010) Does fracture pattern predict death with lateral compression type 1 pelvic fractures? J Trauma 69(4):876–879. doi:10.1097/TA.0b013e3181e785bf
Lau TW, Leung F (2010) Occult posterior pelvic ring fractures in elderly patients with osteoporotic pubic rami fractures. J Orthop Surg (Hong Kong) 18(2):153–157
Kanakaris N, Tzioupis C, Nikolaou V, Giannoudis P (2009) Lateral compression type I injuries of the pelvic ring: are they mechanically stable? Inj Extra 40:183–235. doi:10.1016/j.injury.2009.06.171
Gordon RO, Mears DC (1991) Lateral compression injury of the pelvis. A case report. J Bone Joint Surg Am 73(9):1399–1401
Routt ML Jr, Simonian PT, Ballmer F (1995) A rational approach to pelvic trauma. Resuscitation and early definitive stabilization. Clin Orthop Relat Res 318:61–74
Tile M (1980) Pelvic fractures: operative versus nonoperative treatment. Orthop Clin N Am 11(3):423–464
Tile M (1988) Pelvic ring fractures: should they be fixed? J Bone Joint Surg Br 70(1):1–12
Miranda MA, Riemer BL, Butterfield SL, Burke CJ 3rd (1996) Pelvic ring injuries. A long term functional outcome study. Clin Orthop Relat Res 329:152–159
Bruce B, Reilly M, Sims S (2011) OTA highlight paper predicting future displacement of nonoperatively managed lateral compression sacral fractures: can it be done? J Orthop Trauma 25(9):523–527. doi:10.1097/BOT.0b013e3181f8be33
Mehling I, Hessmann MH, Rommens PM (2012) Stabilization of fatigue fractures of the dorsal pelvis with a trans-sacral bar. Operative technique and outcome. Injury 43(4):446–451. doi:10.1016/j.injury.2011.08.005
Bellabarba C, Ricci WM, Bolhofner BR (2000) Distraction external fixation in lateral compression pelvic fractures. J Orthop Trauma 14(7):475–482
Osterhoff G, Ossendorf C, Wanner GA, Simmen HP, Werner CM (2011) Posterior screw fixation in rotationally unstable pelvic ring injuries. Injury 42(10):992–996. doi:10.1016/j.injury.2011.04.005
Sembler Soles GL, Lien J, Tornetta P 3rd (2012) Nonoperative immediate weightbearing of minimally displaced lateral compression sacral fractures does not result in displacement. J Orthop Trauma 26(10):563–567. doi:10.1097/BOT.0b013e318251217b
Gardner MJ, Parada S, Chip Routt ML Jr (2009) Internal rotation and taping of the lower extremities for closed pelvic reduction. J Orthop Trauma 23(5):361–364. doi:10.1097/BOT.0b013e31819c4a3f
Suzuki T, Morgan SJ, Smith WR, Stahel PF, Flierl MA, Hak DJ (2010) Stress radiograph to detect true extent of symphyseal disruption in presumed anteroposterior compression type I pelvic injuries. J Trauma 69(4):880–885. doi:10.1097/TA.0b013e3181efbad5
Gardner MJ, Krieg JC, Simpson TS, Bottlang M (2010) Displacement after simulated pelvic ring injuries: a cadaveric model of recoil. J Trauma 68(1):159–165. doi:10.1097/TA.0b013e31819adae2
Hoffmann MF, Jones CB, Sietsema DL (2012) Persistent impairment after surgically treated lateral compression pelvic injury. Clin Orthop Relat Res 470(8):2161–2172. doi:10.1007/s11999-012-2247-1
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. No funds were received in support of this study.
Rights and permissions
About this article
Cite this article
Tosounidis, T., Kanakaris, N., Nikolaou, V. et al. Assessment of Lateral Compression type 1 pelvic ring injuries by intraoperative manipulation: which fracture pattern is unstable?. International Orthopaedics (SICOT) 36, 2553–2558 (2012). https://doi.org/10.1007/s00264-012-1685-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-012-1685-4