
Abstract
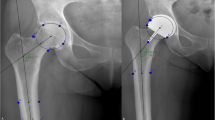
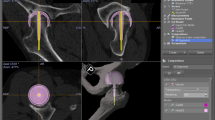
Freehand positioning of the femoral drill guide is difficult during hip resurfacing and the surgeon is often unsure of the implant position achieved peroperatively. The purpose of this study was to find out whether, by using a navigation system, acetabular and femoral component positioning could be made easier and more precise. Eighteen patients operated on by the same surgeon were matched by sex, age, BMI, diagnosis and ASA score (nine patients with computer assistance, nine with the regular ancillary). Pre-operative planning was done on standard AP and axial radiographs with CT scan views for the computer-assisted operations. The final position of implants was evaluated by the same radiographs for all patients. The follow-up was at least 1 year. No difference between both groups in terms of femoral component position was observed (p > 0.05). There was also no difference in femoral notching. A trend for a better cup position was observed for the navigated hips, especially for cup anteversion. There was no additional operating time for the navigated hips. Hip navigation for resurfacing surgery may allow improved visualisation and hip implant positioning, but its advantage probably will be more obvious with mini-incisions than with regular incision surgery.
Résumé
La position du guide fémoral lors du resurfaçage de hanche peut être améliorée par l’utilisation d’un système de navigation. 18 patients comparables en termes de sexe, d’âge, de BMI, de diagnostic et de score ASA ont été opérés par le même chirurgien. 9 patients ont été traités avec l’aide d’un système de navigation et 9 avec le matériel ancillaire habituel sans navigation. L’analyse pré-opératoire et post-opératoire a consisté en une radiographie face profil et un scanner. Le suivi n’a pas été inférieur à un an. Il n’existe pas de différence entre les deux groupes en terme de position fémorale (p > 0.05), il n’y a pas non plus de différence sur les incisions. Par contre, une meilleure position de la cupule a été observée sur les hanches naviguées surtout pour l’anteversion. Il n’y a pas eu d’augmentation du temps opératoire du fait de la navigation. En conclusion, la navigation de la hanche lors d’une intervention chirurgicale de type resurfaçage permet d’avoir une meilleure visualisation de la position des implants mais ces avantages sont plus importants lors d’une mini incision que lors d’une incision classique.
Similar content being viewed by others

References
(1990) EuroQol-a new facility for the measurement of health-related quality of life. The EuroQol Group. Health Policy 16:199–208
Amstutz HC (2006) Hip resurfacing arthroplasty. J Am Acad Orthop Surg 14:452–453
Amstutz HC, Beaule PE, Dorey FJ, Le Duff MJ, Campbell PA, Gruen TA (2004) Metal-on-metal hybrid surface arthroplasty: 2 to 6-year follow-up study. J Bone Joint Surg Am 86-A:28–39
Beaule PE, Amstutz HC, Le Duff M, Dorey F (2004) Surface arthroplasty for osteonecrosis of the hip: hemiresurfacing versus metal-on-metal hybrid resurfacing. J Arthroplasty 19:54–58
Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW (1988) Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol 15:1833–1840
Blendea S, Eckman K, Jaramaz B, Levison TJ, Digioia AM III (2005) Measurements of acetabular cup position and pelvic spatial orientation after total hip arthroplasty using computed tomography/radiography matching. Comput Aided Surg 10:37–43
Cossey AJ, Back DL, Shimmin A, Young D, Spriggins AJ (2005) The nonoperative management of periprosthetic fractures associated with the Birmingham hip resurfacing procedure. J Arthroplasty 20:358–361
Daniel J, Pynsent PB, McMinn DJ (2004) Metal-on-metal resurfacing of the hip in patients under the age of 55 years with osteoarthritis. J Bone Joint Surg Br 86:177–184
De Smet KA, Pattyn C, Verdonk R (2002) Early results pf primary Birmingham hip resurfacing using a hybrid metal-on-metal couple. Hip Int 12:158–162
DeLee JG, Charnley J (1976) Radiological demarcation of cemented sockets in total hip replacement. Clin Orthop Relat Res 20–32
DiGioia AM III, Jaramaz B, Plackeseychuk AY et al (2002) Comparison of a mechanical acetabuar alignment guide with computer placement of the socket. J Arthroplasty 17:359–364
Gruen TA, McNeice GM, Amstutz HC (1979) “Modes of failure” of cemented stem-type femoral components: a radiographic analysis of loosening. Clin Orthop Relat Res 17–27
Harris WH (1969) Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am 51:737–755
Howie DW, Campbell D, McGee M, Cornish BL (1990) Wagner resurfacing hip arthroplasty. The results of one hundred consecutive arthroplasties after 8 to 10 years. J Bone Joint Surg Am 72:708–714
Jolles BM, Genoud P, Hoffmeyer P (2004) Computer-assisted cup placement techniques in total hip arthroplasty improve accuracy of placement. Clin Orthop Relat Res 426:174–179
Jolles BM, Zangger P, Leyvraz PF (2002) Factors predisposing to dislocation after primary total hip arthroplasty: a multivariate analysis. J Arthroplasty 17:282–288
Loughead JM, Chesney D, Holland JP, McCaskie AW (2005) Comparison of offset in Birmingham hip resurfacing and hybrid total hip arthroplasty. J Bone Joint Surg Br 87:163–166
Marti G, Baur C, Zambelli PY (2004) Optimal femoral head contour segmentation in CT images using dynamic programming. Technol Health Care 12:315–322
McCollum DE, Gray WJ (1990) Dislocation after total hip arthroplasty. Causes and prevention. Clin Orthop Relat Res 159–170
McMinn D, Treacy R, Lin K, Pynsent P (1996) Metal on metal surface replacement of the hip. Experience of the McMinn prothesis. Clin Orthop Relat Res S89–S98
McMinn DJ, Roberts P, Forward GR (1991) A new approach to the hip for revision surgery. J Bone Joint Surg Br 73:899–901
Pollard TC, Baker RP, Eastaugh-Waring SJ, Bannister GC (2006) Treatment of the young active patient with osteoarthritis of the hip. A 4- to 7-year comparison of hybrid total hip arthroplasty and metal-on-metal resurfacing. J Bone Joint Surg Br 88:592–600
Pollard TC, Basu C, Ainsworth R, Lai W, Bannister GC (2003) Is the Birmimgham hip resurfacing worthwhile? Hip Int 13:25–28
Treacy RB, McBryde CW, Pynsent PB (2005) Birmingham hip resurfacing arthroplasty. A minimum follow-up of 5 years. J Bone Joint Surg Br 87:167–170
Vail TP (2005) Surface replacement. Advanced reconstruction: hip. American Academy of Orthopaedic Surgeons
Acknowledgments
We thank our data manager Mr Heinrich Ariss.
Author information
Authors and Affiliations
Corresponding author
Additional information
The following authors have designed the study (SK, BMJ), gathered the data (SK, PYZ), analysed the data (SK, PYZ, PFL, BMJ), wrote the initial drafts (SK,BMJ) and ensured the accuracy of the data and analysis (SK, PYZ, PFL, BMJ).
No benefits or funds were received in support of this work. No conflicts of interest are known.
Ethics committee approval was obtained before the beginning of the study.
Rights and permissions
About this article
Cite this article
Krüger, S., Zambelli, P.Y., Leyvraz, PF. et al. Computer-assisted placement technique in hip resurfacing arthroplasty: improvement in accuracy?. International Orthopaedics (SICO 33, 27–33 (2009). https://doi.org/10.1007/s00264-007-0440-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-007-0440-8