
Abstract
Purpose
To determine the incidence of acute kidney injury (AKI), need for emergent dialysis, and renal graft loss in patients with kidney transplants, who underwent CT examinations with low-osmolality iodine-based contrast material (IBCM).
Materials and methods
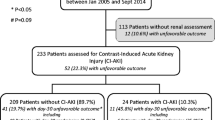
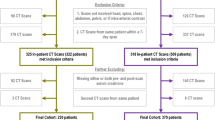
Our institutional review board approved this retrospective Health Insurance Portability and Accountability Act compliant study. From January 2005 to April 2015, a total of 224 CT examinations were performed using low-osmolality IBCM in patients with kidney transplants. Six patients who had septic or cardiogenic shock and 30 patients with documented, failed transplants were excluded from our analysis, yielding a total of 188 examinations. Of these, pre- and post-CT serum creatinine (SCr) values were available for 104 examinations, to allow evaluation of AKI. The mean baseline SCr and estimated glomerular filtration rate (eGFR) in this subgroup were 1.37 mg/dL (median 1.18, range 0.5–6.05) and 65.8 mL/min/1.73 m2, respectively (median 65, range 9–114). AKI was defined as a rise in SCr of either (a) ≥0.3 mg/dL or (b) ≥0.5 mg/dL in the 24- to 72-h period following IBCM administration. For all patients undergoing the 188 examinations, need for dialysis and graft loss 30 days after contrast administration were evaluated.
Results
In patients with pre- and post-CT SCr values, the incidence of AKI was 7% (7/104) based on a rise of ≥0.3 mg/dL and 3% (3/104) based on a rise of ≥0.5 mg/dL. All three patients with the more strict definition (≥0.5 mg/dL) had a pre-CT eGFR <60 mL/min/1.73 m2. No patient required dialysis or had renal graft loss 30 days after contrast administration.
Conclusion
The incidence of AKI after administration of low-osmolality IBCM administration in renal transplant recipients is low, with no instances of emergent dialysis or graft loss at 30 days post contrast.
Similar content being viewed by others

References
Nash K, Hafeez A, Hou S (2002) Hospital-acquired renal insufficiency. Am J Kidney Dis 39(5):930–936
Mehran R, Nikolsky E (2006) Contrast-induced nephropathy: definition, epidemiology, and patients at risk. Kidney Int 69:S11–S15
Ho Y-F, Hsieh K-L, Kung F-L, et al. (2015) Nephrotoxic polypharmacy and risk of contrast medium-induced nephropathy in hospitalized patients undergoing contrast-enhanced CT. Am J Roentgenol 205(4):703–708
Karthikeyan V, Karpinski J, Nair RC, Knoll G (2004) The burden of chronic kidney disease in renal transplant recipients. Am J Transpl 4(2):262–269
Ekberg H, Tedesco-Silva H, Demirbas A, et al. (2007) Reduced exposure to calcineurin inhibitors in renal transplantation. N Engl J Med 357(25):2562–2575
ACR Manual on Contrast Media Version 10.1 (2015).
Haider M, Yessayan L, Venkat K, Goggins M, Patel A, Karthikeyan V (2015) Incidence of contrast-induced nephropathy in kidney transplant recipients. In: Transplantation proceedings, vol 2. Elsevier, pp 379–383
Ahuja T, Niaz N, Agraharkar M (2000) Contrast-induced nephrotoxicity in renal allograft recipients. Clin Nephrol 54(1):11–14
Light JA, Perloff LJ, Etheredge EE, Hill G, Spees EK (1975) Adverse effects of meglumine diatrizoate on renal function in the early post-transplant period. Transplantation 20(5):404–409
Peters C, Delmonico F, Cosimi A, et al. (1983) Risks versus benefits of contrast medium exposure in renal allograft recipients. Surg Gynecol Obstet 156(4):467
McDonald RJ, McDonald JS, Newhouse JH, Davenport MS (2015) Controversies in contrast material–induced acute kidney injury: closing in on the truth? Radiology 277(3):627–632
Davenport MS, Cohan RH, Khalatbari S, Ellis JH (2014) The challenges in assessing contrast-induced nephropathy: where are we now? Am J Roentgenol 202(4):784–789
Rao QA, Newhouse JH (2006) Risk of nephropathy after intravenous administration of contrast material: a critical literature analysis 1. Radiology 239(2):392–397
Stratta P, Bozzola C, Quaglia M (2012) Pitfall in nephrology: contrast nephropathy has to be differentiated from renal damage due to atheroembolic disease. J Nephrol 25(3):282
Katzberg RW, Newhouse JH (2010) Intravenous contrast medium–induced nephrotoxicity: is the medical risk really as great as we have come to believe? 1. Radiology 256(1):21–28
Newhouse JH, Kho D, Rao QA, Starren J (2008) Frequency of serum creatinine changes in the absence of iodinated contrast material: implications for studies of contrast nephrotoxicity. Am J Roentgenol 191(2):376–382
Bruce RJ, Djamali A, Shinki K, et al. (2009) Background fluctuation of kidney function versus contrast-induced nephrotoxicity. Am J Roentgenol 192(3):711–718
McDonald JS, McDonald RJ, Comin J, et al. (2013) Frequency of acute kidney injury following intravenous contrast medium administration: a systematic review and meta-analysis. Radiology 267(1):119–128
Davenport MS, Khalatbari S, Cohan RH, et al. (2013) Contrast material–induced nephrotoxicity and intravenous low-osmolality iodinated contrast material: risk stratification by using estimated glomerular filtration rate. Radiology 268(3):719–728
McDonald RJ, McDonald JS, Bida JP, et al. (2013) Intravenous contrast material–induced nephropathy: causal or coincident phenomenon? Radiology 267(1):106–118
McDonald JS, McDonald RJ, Carter RE, et al. (2014) Risk of intravenous contrast material–mediated acute kidney injury: a propensity score–matched study stratified by baseline-estimated glomerular filtration rate. Radiology 271(1):65–73
McDonald RJ, McDonald JS, Carter RE, et al. (2014) Intravenous contrast material exposure is not an independent risk factor for dialysis or mortality. Radiology 273(3):714–725
Fananapazir G, Troppmann C, Corwin MT, et al. (2016) Incidence of contrast-induced nephropathy after renal graft catheter arteriography using iodine-based contrast medium. Am J Roentgenol 206(4):783–786
McDonald JS, Katzberg RW, McDonald RJ, Williamson EE, Kallmes DF (2015) Is the presence of a solitary kidney an independent risk factor for acute kidney injury after contrast-enhanced CT? Radiology:142676
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Fananapazir, Troppmann, Corwin, Nikpour, Naderi, and Lamba declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional and/or National Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Requirement for informed consent was waived by our Institutional Review Board for this retrospective study.
Rights and permissions
About this article

Cite this article
Fananapazir, G., Troppmann, C., Corwin, M.T. et al. Incidences of acute kidney injury, dialysis, and graft loss following intravenous administration of low-osmolality iodinated contrast in patients with kidney transplants. Abdom Radiol 41, 2182–2186 (2016). https://doi.org/10.1007/s00261-016-0827-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-016-0827-3