
Abstract
Purpose
To investigate the value of dual-energy spectral computed tomographic imaging (DESCT) to predict the origin of carcinomas in the ampullary region.
Materials and methods
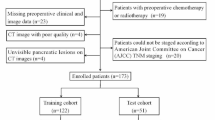
Fifty-seven patients with suspected ampullary region carcinomas underwent DESCT prior to biopsy or surgery. Among those patients, 30 were pancreatic adenocarcinomas, 11 were biliary adenocarcinomas, 16 were adenocarcinomas of the ampulla diagnosed by biopsy and/or pathological examination before or after surgical operation. We compared the CT spectral imaging features among the adenocarcinomas with the above-mentioned three different origins.
Results
Iodine concentration thresholds of 16.36, 21.86, and 21.86 mg/mL yielded a sensitivity and specificity of 100% for distinguishing between common bile duct adenocarcinomas and pancreatic adenocarcinomas in the arterial phase (AP), portal venous phase (PP), and delayed phase (DP), respectively. Thresholds of 16.70, 24.33, and 26.43 mg/mL yielded a sensitivity and specificity of 100% for distinguishing between common bile duct adenocarcinomas and ampullary adenocarcinomas in the AP, PP, and DP, respectively. Iodine concentration thresholds of 16.66 and 17.78 mg/mL yielded a sensitivity and specificity of 100% for distinguishing between ampullary adenocarcinomas and pancreatic adenocarcinomas in the PP and DP, respectively.
Conclusion
DESCT with multiple parameters can provide useful diagnostic information and may be used to predict the histological origin of carcinomas in the ampullary region.





Similar content being viewed by others

Abbreviations
- CECT:
-
Contrast-enhanced CT
- MRI:
-
Magnetic resonance imaging
- DESCT:
-
Dual-energy spectral computed tomography
- MD:
-
Material decomposition
- ROI:
-
Regions of interest
- AP:
-
Arterial phase
- PP:
-
Portal venous phase
- DP:
-
Delayed phase
- ANOVA:
-
Analysis of variance
- ROC:
-
Receiver operating characteristic
- TP:
-
True positive
- TN:
-
True negative
- FP:
-
False positive
- FN:
-
False negative
- AUC:
-
Area under the curve
References
Pham DT, Hura SA, Willmann JK, Nino-Murcia M, Jeffrey RB Jr (2009) Evaluation of periampullary pathology with CT volumetric oblique coronal reformations. AJR 193(3):202–208
Kim JH, Kim M-J, Chung J-J, et al. (2002) Differential diagnosis of periampullary carcinomas at MR Imaging. Radiographics 22(6):1335–1352
Morris-Stiff G, Alabraba E, Tan YM, et al. (2009) Assessment of survival advantage in ampullary carcinoma in relation to tumour biology and morphology. Eur J Surg Oncol 35(7):746–750
Sarmiento JM, Nagomey DM, Sarr MG, Farnell MB (2001) Periampullary cancers: are there difference? Surg Clin North Am 81(3):543–555
Haskell CM, Berek JS (2001) Cancer treatment, 5th edn. Philadelphia: Saunder, pp 800–803
Kim WS, Choi DW, Choi SH, et al. (2012) Clinical significance of pathologic subtype in curatively resected Ampulla of Vater cancer. J Surg Oncol 105(3):266–272
Chan C, Herrera MF, de la Garza L, et al. (1993) Clinical behavior and prognostic factors of periampullary adenocarcinoma. Ann Surg 218(5):632–637
Pickleman J, Koelsch M, Chejfec G (1997) Node-positive duodenal carcinoma is curable. Arch Surg 132(3):241–244
Su CH, Shyr YM, Lui WY, Peng FK (1999) Factors affecting mortality and survival after pancreaticoduodenectomy for carcinoma of the ampulla of Vater. Hepatogastroenterology 46(27):1973–1979
Mugica F, Urdapilleta G, Castiella A, et al. (2007) Selective sphincteroplasty of the papilla in cases at risk due to atypical anatomy. World J Gastroenterol 13(22):3106–3111
Bakaeen FG, Murr MM, Sarr MG, et al. (2000) What prognostic factors are important in duodenal adenocarcinoma? Arch Surg 135(6):635–642
Ahn YJ, Kim SW, Park YC, et al. (2003) Duodenal-preserving resection of the head of the pancreas and pancreatic head resection with second-portion duodenectomy for benign lesions, low-grade malignancies, and early carcinoma involving the periampullary region. Arch Surg 138(2):162–168
Bohra AK, Mckie L, Diamond T (2002) Transduodenal excision of ampullary tumors. Ulster Med J 71(2):121–127
Fong Y, Blumgart LH, Lin E, Fortner JG, Brennan MF (1996) Outcome of treatment for distal bile duct cancer. Br J Surg 83(12):1712–1715
Gourtsoyiannis N, Mako E (1997) Imaging of primary small intestinal tumors by enteroclysis and CT with pathological correlation. Eur Radiol 7(5):625–642
Johnson TRC, Kalender WA (2011) Physical background. In: Johnson TRC, Fink C, Schonberg SO, Reiser MF (eds) Dual energy CT in clinical practice. Berlin: Springer, pp 3–9
Chae EJ, Song J-W, Seo JB, et al. (2008) Clinical utility of dual-energy CT in the evaluation of solitary pulmonary nodules: initial experience. Radiology 249(2):671–681
Acknowledgments
We thank Na Gao, MD, Engineer of GE Healthcare, for technical assistance in this project.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wei, W., Yu, Y., Lv, W. et al. Predictive value of dual-energy spectral computed tomographic imaging on the histological origin of carcinomas in the ampullary region. Abdom Imaging 39, 702–710 (2014). https://doi.org/10.1007/s00261-014-0098-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-014-0098-9