
Abstract
Purpose
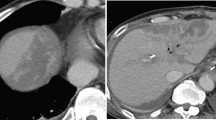
The aim of this CT-based study was to investigate the frequency of splenic infarction (SI) following conventional open gastrectomy performed for gastric malignant neoplasms.
Methods
20 patients who underwent subtotal or total gastrectomy, omentectomy, and D2 lymph node dissections preserving the spleen for gastric malignant neoplasms were retrospectively reviewed. Patients with postoperative CT scans within 3 months were enrolled in this study. CT imaging was performed with a 64-row multidetector CT scanner. Abdominal CT scan with precontrast and postcontrast portal phase images was performed on 19 of the patients, while pulmonary CT angiography was performed on 1 patient for chest pain. Second postoperative control abdominal CT images were also present for 3 of the 5 patients with SI. These examinations were also reviewed for the evolution of the SI’s.
Results
SI was detected in 5 of the patients (25%) at a postoperative early stage. A single infarct area was detected in 4 of the 5 patients while two distinct infarct areas were present in one patient. The infarct areas in two patients disappeared on the second postoperative control CT. A decrease in the size of the SI area in 1 patient was also detected on the second postoperative control CT scan.
Conclusion
The frequency of SI as a complication of abdominal surgeries tends to increase in CT-based studies. We have detected the highest frequency in the literature and suggest that SI, especially when accompanying D2 lymphadenectomy, should be included in the list of early stage gastrectomy complications.





Similar content being viewed by others


References
Ferlay J, Shin HR, Bray F, et al. (2010) Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 127:2893–2917
Songun I, Putter H, Kranenbarg EM, Sasako M, van de Velde CJ (2010) Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol 11:439–449
Ichikawa D, Kurioka H, Yamaguchi T, et al. (2004) Gastric cancer during the last decade. Hepatogastroenterology 51:613–617
Zilberstein B, da Costa Martins B, Jacob CE, et al. (2004) Complications of gastrectomy with lymphadenectomy in gastric cancer. Gastric Cancer 7:254–259
Wilkinson NW, Edwards K, Adams ED (2003) Splenic infarction following laparoscopic Nissen fundoplication: management strategies. JSLS 7:359–365
Robertson F, Leander P, Ekberg O (2001) Radiology of the spleen. Eur Radiol 11:80–95
Skandalakis JE, Gray SW, Rowe JS (1983) Spleen. In: Skandalakis JE, Gray SW, Rowe JS (eds) Anatomical complications in general surgery. New York: McGraw-Hill, pp 179–180
Martinez DG, Sanchez AW, Garcia AP (2008) Splenic abscess after laparoscopic Nissen fundoplication: a consequence of short gastric vessel division. Surg Laparosc Endosc Percutan Tech 18:82–85
Antopolsky M, Hiller N, Salameh S, Goldshtein B, Stalnikowicz R (2009) Splenic infarction: 10 years of experience. Am J Emerg Med 27:262–265
Taylor AJ, Dodds WJ, Erickson SJ, Stewart ET (1991) CT of acquired abnormalities of the spleen. AJR Am J Roentgenol 157:1213–1219
Rabushka LS, Kawashima A, Fishman EK (1994) Imaging of the spleen: CT with supplemental MR examination. Radiographics 14:307–332
Chew HK, Wun T, Harvey D, Zhou H, White RH (2006) Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch Intern Med 166:458–464
Heit JA, Silverstein MD, Mohr DN, et al. (2000) Risk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control study. Arch Intern Med 160:809–815
Ipek T, Eyuboglu E, Ozben V (2010) Partial splenic infarction as a complication of laparoscopic floppy nissen fundoplication. J Laparoendosc Adv Surg Tech A 20:333–337
Hwang SH, Park do J, Jee YS, et al. (2009) Actual 3-year survival after laparoscopy-assisted gastrectomy for gastric cancer. Arch Surg 144:559–564
Stamou KM, Menenakos E, Gomatos IP, Panousopoulos SG, Smparounis S, Leandros E, Zografos G (2010) Clinical implications of sleeve gastrectomy as a source of spleen infarction or ischemia. Obes Surg. doi: 10.1007/s11695-010-0302-0
Ring A, Stein E, Stern J (2009) Splenic ınfarct—an unusual complication of gastrectomy for cardia carcinoma. Internet J Surg 21(1)
Barzilai M, Schlag-Eisenberg D, Peled N, Bitterman A (2000) Noninfectious gas accumulation in an infarcted spleen. Dig Surg 17:402–404
Lawrence W (1993) Total gastrectomy. In: Daly JM, Cady B (eds) Atlas of surgical oncology. St. Louis: Mosby, pp 241–261
Nores M, Phillips EH, Morgenstern L, Hiatt JR (1998) The clinical spectrum of splenic infarction. Am Surg 64:182–188
Freeman JL, Jafri SZ, Roberts JL, Mezwa DG, Shirkhoda A (1993) CT of congenital and acquired abnormalities of the spleen. Radiographics 13:597–610
Yu J, Turner MA, Cho SR, et al. (2004) Normal anatomy and complications after gastric bypass surgery: helical CT findings. Radiology 231:753–760
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Akin, K., Kosehan, D., Cengiz, A.Y. et al. Splenic infarction following conventional open gastrectomy in patients with gastric malignancy: a CT-based study. Abdom Imaging 37, 609–615 (2012). https://doi.org/10.1007/s00261-011-9812-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-011-9812-z