
Abstract
Purpose
To investigate the impact of PET and PET/CT scanning on decision-making in management planning and to identify the optimal setting for selecting candidates for surgery in suspicious recurrent ovarian cancer.
Methods
A retrospective chart review was performed in patients with possible recurrent ovarian cancer after primary optimal cytoreduction and taxane/carboplatin chemotherapy who had undergone FDG PET or FDG PET/CT scans from July 2002 to August 2008 to help make treatment decisions. The analysis included 44 patients who had undergone a total of 89 PET scans. The positive PET scans were classified as follows. (1) localized (one or two localized sites of FDG uptake), (2) multiple (three or more sites of FDG uptake), (3) diffuse (extensive low-grade activity outlining serosal and peritoneal surfaces).
Results
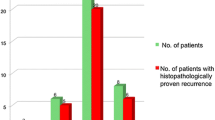
Of the 89 PET scans, 52 (58.4 %) led to a change in management plan. The total number of patients in whom cytoreductive surgery was selected as the treatment of choice increased from 12 to 35. Miliary disseminated disease, which was not detected by PET scan, was found in 22.2 % of those receiving surgery. Miliary disseminated disease was detected in 6 of the 12 patients with recurrent disease whose treatment-free interval (TFI) was <12 months, whereas none of those with a TFI of ≥12 months had such disease (P = 0.0031).
Conclusion
PET or PET/CT is useful for selecting candidates for cytoreductive surgery among patients with recurrent ovarian cancer. To avoid surgical attempts in those with miliary dissemination, patients with a TFI of ≥12 months are the best candidates for cytoreductive surgery.

Similar content being viewed by others

References
Chi DS, McCaughty K, Diaz JP, Huh J, Schwabenbauer S, Hummer AJ, et al. Guidelines and selection criteria for secondary cytoreductive surgery in patients with recurrent, platinum-sensitive epithelial ovarian carcinoma. Cancer. 2006;106:1933–9.
Salani R, Santillan A, Zahurak ML, Giuntoli 2nd RL, Gardner GJ, Armstrong DK, et al. Secondary cytoreductive surgery for localized, recurrent epithelial ovarian cancer: analysis of prognostic factors and survival outcome. Cancer. 2007;109:685–91.
Bristow RE, Puri I, Chi DS. Cytoreductive surgery for recurrent ovarian cancer: a meta-analysis. Gynecol Oncol. 2009;112:265–74.
Hising C, Anjegard IM, Einhorn N. Clinical relevance of the CA 125 assay in monitoring of ovarian cancer patients. Am J Clin Oncol. 1991;14:111–4.
Zanaboni F, Presti M, Scarfone G, Bolis G. CA 125 reliability in predicting ovarian cancer recurrence. Tumori. 1989;75:69–71.
Rustin GJ, van der Burg ME, Griffin CL, Guthrie D, Lamont A, Jayson GC, et al. Early versus delayed treatment of relapsed ovarian cancer (MRC OV05/EORTC 55955): a randomised trial. Lancet. 2010;376:1155–63.
Tanner EJ, Chi DS, Eisenhauer EL, Diaz-Montes TP, Santillan A, Bristow RE. Surveillance for the detection of recurrent ovarian cancer: survival impact or lead-time bias? Gynecol Oncol. 2010;117:336–40.
Rustin GJ, Nelstrop AE, Tuxen MK, Lambert HE. Defining progression of ovarian carcinoma during follow-up according to CA 125: a North Thames Ovary Group Study. Ann Oncol. 1996;7:361–4.
Ferrozzi F, Bova D, De Chiara F, Garlaschi G, Draghi F, Cocconi G, et al. Thin-section CT follow-up of metastatic ovarian carcinoma correlation with levels of CA-125 marker and clinical history. Clin Imaging. 1998;22:364–70.
Garcia-Velloso MJ, Jurado M, Ceamanos C, Aramendia JM, Garrastachu MP, Lopez-Garcia G, et al. Diagnostic accuracy of FDG PET in the follow-up of platinum-sensitive epithelial ovarian carcinoma. Eur J Nucl Med Mol Imaging. 2007;34:1396–405.
Simcock B, Neesham D, Quinn M, Drummond E, Milner A, Hicks RJ. The impact of PET/CT in the management of recurrent ovarian cancer. Gynecol Oncol. 2006;103:271–6.
Sebastian S, Lee SI, Horowitz NS, Scott JA, Fischman AJ, Simeone JF, et al. PET-CT vs CT alone in ovarian cancer recurrence. Abdom Imaging. 2008;33:112–8.
Limei Z, Yong C, Yan X, Shuai T, Jiangyan X, Zhiqing L. Accuracy of positron emission tomography/computed tomography in the diagnosis and restaging for recurrent ovarian cancer: a meta-analysis. Int J Gynecol Cancer. 2013;23:598–607.
Soussan M, Wartski M, Cherel P, Fourme E, Goupil A, Le Stanc E, et al. Impact of FDG PET-CT imaging on the decision making in the biologic suspicion of ovarian carcinoma recurrence. Gynecol Oncol. 2008;108:160–5.
Mangili G, Picchio M, Sironi S, Vigano R, Rabaiotti E, Bornaghi D, et al. Integrated PET/CT as a first-line re-staging modality in patients with suspected recurrence of ovarian cancer. Eur J Nucl Med Mol Imaging. 2007;34:658–66.
Fulham MJ, Carter J, Baldey A, Hicks RJ, Ramshaw JE, Gibson M. The impact of PET-CT in suspected recurrent ovarian cancer: a prospective multi-centre study as part of the Australian PET Data Collection Project. Gynecol Oncol. 2009;112:462–8.
Shih KK, Chi DS, Barakat RR, Leitao Jr MM. Tertiary cytoreduction in patients with recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer: an updated series. Gynecol Oncol. 2010;117:330–5.
Palomar A, Nanni C, Castellucci P, Ambrosini V, Montini GC, Allegri V, et al. Value of FDG PET/CT in patients with treated ovarian cancer and raised CA125 serum levels. Mol Imaging Biol. 2012;14:123–9.
Rose PG, Faulhaber P, Miraldi F, Abdul-Karim FW. Positive emission tomography for evaluating a complete clinical response in patients with ovarian or peritoneal carcinoma: correlation with second-look laparotomy. Gynecol Oncol. 2001;82:17–21.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ebina, Y., Watari, H., Kaneuchi, M. et al. Impact of FDG PET in optimizing patient selection for cytoreductive surgery in recurrent ovarian cancer. Eur J Nucl Med Mol Imaging 41, 446–451 (2014). https://doi.org/10.1007/s00259-013-2610-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-013-2610-9