
Abstract
Purpose
We conducted a pilot trial to evaluate the value of 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography (PET) in gestational trophoblastic tumours (GTTs).
Methods
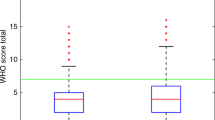
Patients with placental site trophoblastic tumour (PSTT), high-risk GTT (World Health Organisation score ≥8, disease onset at postpartum or greater than 6 months after antecedent pregnancy), metastatic GTT, recurrent/resistant GTT after chemotherapy, or post-molar GTT with unexplained abnormal β-hCG regression and patients undergoing re-evaluation after salvage treatment were enrolled. PET was undertaken within 1 week after computed tomography (CT). Clinical impacts of additional PET were determined on a scan basis.
Results
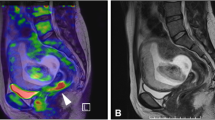
A total of 14 patients were recruited. Sixteen PET scans were performed, with one patient having three serial studies. Benefits of additional PET were seen in 7 of 16 (43.8%) scans; these benefits included disclosure of chemotherapy-resistant lesions (n=2), exclusion of false-positive CT lesions (n=1), detection of an additional lesion not found by conventional imaging (n=1) in high-risk GTT at the start of primary chemotherapy, and confirmation of complete response to treatment for PSTT or to salvage therapy for recurrent/resistant GTT (n=3). On the other hand, in two instances there were false-negative PET findings, six scans yielded no benefit, and one showed an indeterminate lesion.
Conclusion
Our preliminary results suggest that 18F-FDG PET is potentially useful in selected patients with GTT by providing precise mapping of metastases and tumour extent upfront, by monitoring treatment response and by localising viable tumours after chemotherapy. A larger study is necessary to further define the role of 18F-FDG PET in GTT.


Similar content being viewed by others

References
Bower M, Newlands ES, Holden L, Short D, Rustin GJ, Begent RH, et al. EMA/CO for high-risk gestational trophoblastic tumours: results from a cohort of 272 patients. J Clin Oncol 1997;15:2636–43
Lehman E, Gershenson DM, Burke TW, Levenback C, Silva EG, Morris M. Salvage surgery for chemorefractory gestational trophoblastic disease. J Clin Oncol 1994;12:2737–42
Newlands ES, Bower M, Holden L, Short D, Seckl MJ, Rustin GJ, et al. Management of resistant gestational trophoblastic tumours. J Reprod Med 1998;43:111–8
Feltmate CM, Genest DR, Wise L, Berstein MR, Goldstein DP, Berkowitz RS. Placental site trophoblastic tumour: a 17-year experience at the New England Trophoblastic Disease Center. Gynecol Oncol 2001;82:415–9
Hricak H, Demas BE, Braga CA, Fisher MR, Winkler ML. Gestational trophoblastic neoplasm of the uterus: MR assessment. Radiology 1986;161:11–6
Hillard AE, Allen RW, Beale G. Metastatic choriocarcinoma: correlation of MRI, CT, and angiography. South Med J 1993;86:1299–302
Gambhir SS, Czenin J, Schwimmer J, Silverman DHS, Coleman RE, Phelps MW. A tabulated summary of the FDG PET literature. J Nucl Med 2001;42:1S–93S
Yen TC, Ng KK, Ma SY, Chou HH, Tsai CS, Hsueh S, et al. Value of dual-phase 2-fluoro-2-deoxy-d-glucose positron emission tomography in cervical cancer. J Clin Oncol 2003;21:3651–8
Chang TC, Law KS, Hong JH, Lai CH, Yen TC, Ng KK, et al. Positron emission tomography for unexplained serum SCC-Ag elevation in cervical cancer patients—a phase II study. Cancer 2004;101:164–71
Hebart H, Erley C, Kaskas B, Mayer R, Konig M, Einsele H, et al. Positron emission tomography helps to diagnose tumour emboli and residual disease in choriocarcinoma. Ann Oncol 1996;7:416–8
Truenbach J, Pereira PL, Huppert PE, Farnsworth C, Mayer R, Feline U, et al. Primary choriocarcinoma of the pulmonary artery mimicking pulmonary embolism. Br J Radiol 1997;70:843–5
Zhuang H, Yamamoto AJ, Ghesani N, Alavi A. Detection of choriocarcinoma in the lung by FDG positron emission tomography. Clin Nucl Med 2001;26:723
Dose J, Bohuslavizki K, Huneke B, Lindner C, Janicke F. Detection of intramural choriocarcinoma of the uterus with 18F-FDG-PET. A case report. Clin Positron Imaging 2000;3:37–40
Sironi S, Picchio M, Mangili G, Garavaglia E, Zangheri B, Messa C, et al. [18F]fluorodeoxyglucose positron emission tomography as a useful indicator of metastatic gestational trophoblastic tumour: preliminary results in three patients. Gynecol Oncol 2003;91:226–30
Bagshawe KD. Choriocarcinoma. A model for tumour markers. Acta Oncol 1992;31:99–106
World Health Organization. Gestational trophoblastic diseases. WHO Technical Report Series. Switzerland: WHO; 1983. p. 692
Mutch DG, Soper JT, Babcock CJ, Clerke-Pearson DL, Hammond CB. Recurrent gestational trophoblastic disease. Experience of the Southern Regional Trophoblastic Disease Center. Cancer 1990;66:978–82
Tsai CC, Tsai CS, Ng KK, Ma SY, Chou HH, Tsai CS, et al. The impact of image fusion in resolving discrepant findings between FDG-PET and MRI/CT in patients with gynaecological cancers. Eur J Nucl Med Mol Imaging 2003;30:1674–83
Matsui H, Suzuka K, Litsuka Y, Yamazawa K, Tanaka N, Mitsuhashi A, et al. Salvage combination chemotherapy with 5-fluorouracil and actinomycin D for patients with refractory, high-risk gestational trophoblastic tumours. Cancer 2002;95:1051–4
Chen LP, Cai SM, Fan JX, Li ZT. PEBA regimen (cisplatin, etoposide, bleomycin, and adriamycin) in the treatment of drug-resistant choriocarcinoma. Gynecol Oncol 1995;56:231–4
Lotz JP, Andre T, Donsimori R, Firmin C, Bouleuc C, Bonnak H, et al. High dose chemotherapy with ifosfamide, carboplatin, and etoposide combined with autologous bone marrow transplantation for the treatment of poor-prognosis germ cell tumours and metastatic trophoblastic disease in adults. Cancer 1995;75:874–85
Rustin GJS, Newlands ES, Begent RHJ, Dent J, Bagshawe KD. Weekly alternating etoposide, methotrexate, and actinomycin/vincristine and cyclophosphamide chemotherapy for the treatment of CNS metastases of choriocarcinoma. J Clin Oncol 1989;7:900–3
Schechter NR, Mychalczak B, Jones W, Spriggs D. Prognosis of patients treated with whole brain radiation therapy for metastatic gestational trophoblastic disease. Gynecol Oncol 1998;68:183–92
Ngan HY, Chan FL, Au VWK, Cheng DKL, Ng TY, Wong LC. Clinical outcome of micrometastasis in the lung in stage IA persistent gestational trophoblastic disease. Gynecol Oncol 1998;70:192–4
Gillespie AM, Kumar S, Hancock BW. Treatment of persistent trophoblastic diease later than 6 months after diagnosis of molar pregnancy. Br J Cancer 2000;82:1393–5
Acknowledgements
This work was supported by grants from Chang Gung Memorial Hospital (CTRP 91-017) and the National Science Council of Taiwan (NSC 91-2314-B-182A-157 and NSC 92-2314-B-182A-184).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chang, T.C., Yen, T.C., Li, Y.T. et al. The role of 18F-fluorodeoxyglucose positron emission tomography in gestational trophoblastic tumours: a pilot study. Eur J Nucl Med Mol Imaging 33, 156–163 (2006). https://doi.org/10.1007/s00259-005-1873-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-005-1873-1