
Abstract
Objective
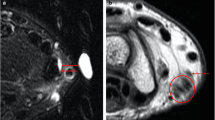
De Quervain tenosynovitis affects the first extensor compartment of the wrist and occurs more frequently in females. This high prevalence could not be explained by soft tissue. As the osseous anatomy has been mostly neglected, we aimed to compare the distal radius between the sexes.
Materials and methods
We evaluated the presence of a bony ridge on the floor of the first extensor compartment on CT images with multiplanar imaging.
Results
We included 244 wrists (72 females, 172 males) in the study. A bony ridge was present in 58 (23.8 %) and absent in 186 (76.2 %) wrists. A ridge was present in 24 (33.3 %) wrists among females and 34 (19.8 %) wrists among males. A groove with a bony ridge was statistically associated with females.
Conclusion
We observed two tendon groove morphologies for the first extensor compartment. A groove with a bony ridge occurs more frequently in females. Further research is needed to clarify the relationship between the high frequency of a bony ridge and increased prevalence of de Quervain tenosynovitis in females.


Similar content being viewed by others


References
Dang AC, Rodner CM. Unusual compression neuropathies of the forearm, part I: radial nerve. J Hand Surg [Am]. 2009;34:1906–14.
Ilyas A, Ast M, Schaffer AA, Thoder J. De Quervain tenosynovitis of the wrist. J Am Acad Orthop Surg. 2007;15:757–64.
Kay NRM. De Quervain’s disease: changing pathology or changing perception? J Hand Surg (Br). 2000;25:65–9.
Clarke MT, Lyall HA, Grant JW, Matthewson MH. The histopathology of de Quervain’s disease. J Hand Surg (Br). 1998;23:732–4.
Volpe A, Pavoni M, Marchetta A, et al. Ultrasound differentiation of two types of de Quervain’s disease: the role of retinaculum. Ann Rheum. 2010;69:938–9.
Petit Le Manac’h A, Roquelaure Y, Ha C, et al. Risk factors for de Quervain’s disease in a French working population. Scand J Work Environ Health. 2011;37:394–401.
Tanaka S, Petersen M, Cameron L. Prevalence and risk factors of tendinitis and related disorders of the distal upper extremity among US workers: comparison to carpal tunnel syndrome. Am J Ind Med. 2001;39:328–35.
Walker-bone K, Palmer KT, Reading I, Coggon D, Cooper C. Prevalence and impact of musculoskeletal disorders of the upper limb in the general population. Arthritis Rheum. 2004;51:642–51.
Wolf JM, Sturdivant RX, Owens BD. Incidence of de Quervain tenosynovitis in a young, active population. J Hand Surg [Am]. 2009;34:112–5.
Stahl S, Vida D, Meisner C, Stahl AS, Schaller HE, Held M. Work related etiology of de Quervain’s tenosynovitis: a case–control study with prospectively collected data. BMC Musculoskelet Disord. 2015;16:126.
Alemohammad AM, Yazaki N, Morris RP, Buford WL, Viegas SF. Thumb interphalangeal joint extension by the extensor pollicis brevis: association with a subcompartment and de Quervain’s disease. J Hand Surg [Am]. 2009;34:719–23.
Gousheh J, Yavari M, Arasteh E. Division of the first dorsal compartment of the hand into two separated canals: rule or exception? Arch Iran Med. 2009;12:52–4.
Harvey FJ, Harvey PM, Horsley MW. De Quervain’s disease: surgical or nonsurgical treatment. J Hand Surg [Am]. 1990;15:83–7.
Jackson WT, Viegas SF, Coon TM, Stimpson KD, Frogameni AD, Sımpson JM. Anatomical variations in the first extensor compartment of the wrist. J Bone Joint Surg Am. 1986;68:923–6.
Minamikawa Y, Peimer CA, Cox WL, Sherwin FS. De Quervain’s syndrome: surgical and anatomical studies of the fibroosseous canal. Orthopedics. 1991;14:545–9.
Richie CA, Brimer WW. Corticosteroid injection for treatment of de Quervain’s tenosynovitis: a pooled quantitative literature evaluation. J Am Board Fam Pract. 2003;16:102–6.
Witt J, Pess G, Gelberman RH. Treatment of de Quervain’s tenosynovitis. A prospective study of the results of injection of steroids and immobilization in a splint. J Bone Joint Surg Am. 1991;73:219–22.
De Keating-Hart E, Touchais S, Kerjean Y, Ardouin L, Le Goff B. Presence of an intracompartmental septum detected by ultrasound is associated with the failure of ultrasound-guided steroid injection in de Quervain’s syndrome. J Hand Surg Eur Vol. 2015. doi:10.1177/1753193415611414.
Kulthanan T, Chareonwat B. Variations in abductor pollicis longus and extensor pollicis brevis tendons in the Quervain syndrome: a surgical and anatomical study. Scand J Plast Reconstr Surg Hand Surg. 2007;41:36–8.
Mirzanli C, Ozturk K, Esenyel CZ, Ayanoglu S, Imren Y, Aliustaoglu S. Accuracy of intrasheath injection techniques for de Quervain’s disease: a cadaveric study. J Hand Surg Eur Vol. 2012;37:155–60.
Motoura H, Shiozaki K, Kawasaki K. Anatomical variations in the tendon sheath of the first compartment. Anat Sci Int. 2010;85:145–51.
Nayak SR, Hussein M, Krishnamurthy A, et al. Variation and clinical significance of extensor pollicis brevis: a study in South Indian cadavers. Chang Gang Med J. 2009;32:600–4.
Shiraishi N, Matsumura G. Anatomical variations of the extensor pollicis brevis tendon and abductor pollicis tendon. Relation to tenosynovectomy. Okajimas Folia Anat Jpn. 2005;82:25–9.
Mahakkanukrauh P, Mahakkanukrauh C. Incidence of a septum in the first dorsal compartment and its effects on therapy of de Quervain’s disease. Clin Anat. 2000;13:195–8.
Rousset P, Vuillemin-Bodaghi V, Laredo JD, Parlier-Cuau C. Anatomic variations in the first extensor compartment of the wrist: accuracy of US. Radiology. 2010;257:427–33.
Xiao L, Li YK, Ye GH, Yang XW. Variations in the extensor grooves on the radial styloid process in Chinese population. Surg Radiol Anat. 2012;35:49–53.
Gurses IA, Coskun O, Gayretli O, Kale A, Ozturk A. The anatomy of the fibrous and osseous components of the first extensor compartment of the wrist: a cadaveric study. Surg Radiol Anat. 2015;37:773–7.
Lee KH, Kang CN, Lee BG, Jung WS, Kim DY, Lee CH. Ultrasonographic evaluation of the first extensor compartment of the wrist in de Quervain’s disease. J Orthop Sci. 2014;19:49–54.
Choi SJ, Ahn JH, Lee YJ, et al. De Quervain disease: US identification of anatomic variations in the first extensor compartment with an emphasis on subcompartmentalization. Radiology. 2011;260:480–6.
Glajchen N, Schweitzer M. MRI features in de Quervain’s tenosynovitis of the wrist. Skelet Radiol. 1996;25:63–5.
Hadidy A, Hadidy S, Haroun A, et al. De Quervain’s tenosynovitis imaging: ultrasonography versus magnetic resonance imaging. J Bahrain Med Soc. 2009;21:328–31.
Stahl S, Vida D, Meisner C, et al. Systematic review and meta-analysis on the work-related cause of de Quervain tenosynovitis: a critical appraisal of its recognition as an occupational disease. Plast Reconstr Surg. 2013;132:1479–91.
Acknowledgments
We wish to thank David F. Chapman, BSc., for editing the English of our article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Institutional Review Board approval (no: 2015/08/07 date: 11.05.2015) for the study was obtained.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that they have no conflict of interests.
Rights and permissions
About this article

Cite this article
Gurses, I.A., Turkay, R., Inci, E. et al. Sex differences in the radial grooves in the first extensor compartment. Skeletal Radiol 45, 955–958 (2016). https://doi.org/10.1007/s00256-016-2381-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-016-2381-z