
Abstract
Objective
To determine the imaging features of hemosiderotic fibrolipomatous tumor (HFLT), which has a propensity towards local recurrence and the potential to transform into myxoinflammatory fibroblastic sarcoma (MIFS).
Materials and methods
The study included 8 patients with a diagnosis of HFLT and imaging at a tertiary cancer center. Imaging studies included radiographs (n = 2), ultrasound (n = 3), and MRI (n = 16). Imaging features were evaluated including location, calcification, sonographic echogenicity, vascular flow, size, border, signal characteristics, contrast enhancement, and blooming on MRI.
Results
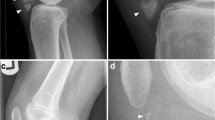
The HFLT was located in the ankle/foot in 4 out of 8 and was subcutaneous in 8 out of 8, ranging in size from 2 to 18 cm. Histology at initial diagnosis was HFLT in 5 out of 8 and HFLT with MIFS in 3 out of 8. None was calcified on radiography. On ultrasound 2 out of 3 were heterogeneously echogenic with ≥10 foci of vascular flow. Two out of 8 patients had MRI only at local recurrence. The tumor border was infiltrative in 4 out of 6 at initial diagnosis and in 2 patients with MRI at recurrence only. Fat and septae were present in 7 out of 8 at initial diagnosis and at recurrence. Signal intensity was iso-/hypointense to muscle on T1-weighted sequences in more than two thirds of the tumor in 4 out of 7 and hyperintense to muscle in at least one third of the tumor on fluid-sensitive sequences in 6 out of 8. Contrast enhancement was heterogeneous in 7 out of 7; blooming in two thirds of the tumor on gradient-echo sequence MRI indicated hemorrhage.
Conclusion
The HFLT commonly presents as a mass with an infiltrative border, interspersed fat and septations at initial diagnosis and local recurrence on MRI regardless of histology of HFLT alone or with MIFS. Hemosiderin deposits may be detected as blooming on gradient-echo sequences.




Similar content being viewed by others


References
Browne TJ, Fletcher CD. Haemosiderotic fibrolipomatous tumor (so-called haemosiderotic fibrohistiocytic lipomatous tumor): analysis of 13 new cases in support of a distinct entity. Histopathology. 2006;48:453–61.
Moretti VM, Brooks JS, Ogilvie CM. Case report: hemosiderotic fibrohistiocytic lipomatous lesion: a clinicopathologic characterization. Clin Orthop Relat Res. 2010;468(10):2808–13.
Antonescu CR, Link TM, O'Donnell RJ, Folpe AL, Horvai AE. Hemosiderotic fibrolipomatous tumor, not an entirely benign entity. Solomon DA. Am J Surg Pathol. 2013;37(10):1627–30.
Marshall-Taylor C, Fanburg-Smith JC. Hemosiderotic fibrohistiocytic lipomatous lesion: ten cases of a previously undescribed fatty lesion of the foot ⁄ ankle. Mod Pathol. 2000;13:1192–9.
De Vreeze RS, Koops W, Haas RL, van Coevorden F. An unusual case of hemosiderotic fibrohistiocytic lipomatous lesion: correlation of MRI and pathologic findings. Sarcoma. 2008;2008:893918.
West AT, Toms AP, Murphy J, Sultan M. Haemosiderotic fibrohistiocytic lipomatous lesion/tumor of the foot: MRI and histopathology. Skeletal Radiol. 2008;37:71–4.
Hallor KH, Sciot R, Staaf J, Heidenblad M, et al. Two genetic pathways, t(1;10) and amplification of 3p11–12, in myxoinflammatory fibroblastic sarcoma, haemosiderotic fibrolipomatous tumor, and morphologically similar lesions. J Pathol. 2009;217:716–27.
Kazakov DV, Sima R, Michal M. Hemosiderotic fibrohistiocytic lipomatous lesion: clinical correlation with venous stasis. Virchows Arch. 2005;447:103–6.
Luzar B, Gasljevic G, Juricic V, Bracko M. Hemosiderotic fibrohistiocytic lipomatous lesion: early pleomorphic hyalinising angiectatic tumor? Pathol Int. 2006;56:283–6.
Wettach GR, Boyd LJ, Lawce HJ, Magenis RE, Mansoor A. Cytogenetic analysis of a hemosiderotic fibrolipomatous tumor. Cancer Genet Cytogenet. 2008;182:140–3.
Prud’homme A, Rousselot C, de Pinieux G, Voche P, Rosset P. Tumeurs fibrolipomateuses hémosidérotiques: une nouvelle entité à ne pas méconnaître [Hemosiderotic fibrohistiocytic lipomatous lesion: a new entity you must remind]. Ann Chir Plast Esthet. 2007;52(6):616–20.
Guillou L, Coindre JM. Newly described adipocytic lesions. Semin Diagn Pathol. 2001;18(4):238–49.
Michal M, Kazakov DV. Relationship between pleomorphic hyalinizing angiectatic tumor and hemosiderotic fibrohistiocytic lipomatous lesion. Am J Surg Pathol. 2005;29(9):1256–7; author reply 1259.
Folpe AL, Weiss SW. Pleomorphic hyalinizing angiectatic tumor: analysis of 41 cases supporting evolution from a distinctive precursor lesion. Am J Surg Pathol. 2004;28(11):1417–25.
Antonescu CR, Zhang L, Nielsen GP, et al. Consistent t(1;10) with rearrangements of TGFBR3 and MGEA5 in both myxoinflammatory fibroblastic sarcoma and hemosiderotic fibrolipomatous tumor. Genes Chromos Cancer. 2011;50:757–84.
Meis-Kindblom JM, Kindblom LG. Acral myxoinflammatory fibroblastic sarcoma: a low-grade tumor of the hands and feet. Am J Surg Pathol. 1998;22:911–24.
Michal M. Inflammatory myxoid tumor of the soft parts with bizarre giant cells. Pathol Res Pract. 1998;194:529–33.
Montgomery EA, Devaney KO, Giordano TJ, Weiss SW. Inflammatory myxohyaline tumor of distal extremities with virocyte or Reed-Sternberg-like cells: a distinctive lesion with features simulating inflammatory conditions, Hodgkin’s disease, and various sarcomas. Mod Pathol. 1998;11:384–91.
Lim R, Jaramillo D, Poussaint TY, Chang Y, Korf B. Superficial neurofibroma: a lesion with unique MRI characteristics in patient with neurofibromatosis type 1. AJR Am J Roentgenol. 2005;184(3):962–8.
Conflict of interest
No conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
O’Driscoll, D., Athanasian, E., Hameed, M. et al. Radiological imaging features and clinicopathological correlation of hemosiderotic fibrolipomatous tumor: experience in a single tertiary cancer center. Skeletal Radiol 44, 641–648 (2015). https://doi.org/10.1007/s00256-014-2078-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-014-2078-0