
Abstract
Objective
To assess the MR imaging features of spindle cell lipomas (SCL) and to compare these appearances directly with the histopathological findings.
Materials and methods
A retrospective review of our soft tissue tumor database was performed. This yielded 1,327 histologically proven lipomas, of which 25 were confirmed as being SCLs. Fourteen of the 25 patients had MR examinations available for review and only these patients were included in our study. Lesions were assessed at MR examination for the degree of internal fat signal content with grade 0 representing 0 % fat signal and grade 4 100 % fat signal. The degree of fat suppression and contrast-enhancement pattern were also recorded. The excision specimens were independently reviewed by a consultant histopathologist. The histology specimens were assessed for the amount of internal fat and non-adipose tissue and graded using the same scale applied for the imaging. Where core needle biopsy (CNB) was performed, the CNB specimens were also examined for positive features of SCL.
Results
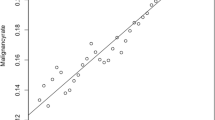
In our study, 93 % (13/14) of our patients were male and the average age was 58 years. 65 % (9/14) of the lesions presented in the upper back, shoulder, or neck. All lesions were subcutaneous. 35 % (5/14) of the SCLs demonstrated grade 3 (>75 %) or grade 4 (100 %) fat signal on MR examination. 35 % (5/14) of the lesions had grade 2 (25–75 %) fat signal and 29 % (4/14) of the lesions demonstrated grade 0 (0 %) or grade 1 (<25 %) fat signal. 43 % (6/14) of lesions demonstrated homogenous fat suppression, 28 % (4/14) showed focal areas of high internal signal, and 28 % (4/14) had diffuse internal high signal on fluid-sensitive fat-saturated sequences. 86 % (6/7) of the cases demonstrated septal/nodular enhancement. The diagnosis was evident on the CNB specimen in 100 % (9/9) cases. The histopathology fat content grade was in agreement with the imaging grade in 86 % (12/14) cases.
Conclusions
The internal signal pattern of SCL can range broadly, with low fat content lesions seen almost as commonly as intermediate and high fat content lesions. We also found that the fat:non-fat internal MR signal pattern of these lesions is accurately reflected in their composition at histology.







Similar content being viewed by others


References
Enzinger FM, Harvey DA. Spindle cell lipoma. Cancer. 1975;36:1852–9.
Kransdorf MJ, Murphey MD. Imaging of soft tissue tumours. Philadelphia: Saunders; 1997. p. 3–35.
Bancroft LW et al. Imaging characteristics of spindle cell lipoma. Am J Radiol. 2003;181:1251–4.
Choi JW et al. Spindle cell lipoma of the head and neck: CT and MR imaging findings. Neuroradiology. 2013;55:101–6.
Bui-Mansfield LT, Kaplan KJ. Spindle cell lipoma of the upper back. Am J Radiol. 2002;179:1158.
Braunschweig IJ et al. Case report 751: Spindle cell lipoma causing marked bone erosion. Skeletal Radiol. 1992;21:414–7.
Christopher D, Unni K, Mertens F. Adipocytic Tumors. WHO Classification of Tumors. Pathology and Genetics: Tumors of Soft Tissue and Bone. Lyon: IARC; 2002. p. 19–46.
Murphey MD et al. Benign musculoskeletal lipomatous lesions. Radiographics. 2004;24:1433–66.
Weis SW, Goldblum JR. Benign lipomatous tumours. In: Weis SW, Goldblum JR, editors. Enzinger and Weiss’s soft tissue tumours. 4th ed. St. Louis: Mosby; 2001. p. 571–639.
Tosios K et al. Spindle cell lipoma of the oral cavity. Int J Oral Maxillofac Surg. 1995;24:363–4.
Haas N et al. Spindle cell lipoma of the scalp: a case report and review. Derm Surg. 1999;25:68–71.
Ide H, Nakagawa T, Kamiyama Y, Muto S, Imamura T, Horie S. Spindle cell lipoma of the spermatic cord. Int J Urol. 2007;14:1046–7.
Sund S et al. Large intramuscular spindle-cell lipoma: a case report. APMIS. 1988;96:347–51.
Conflict of interest
The authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kirwadi, A., Abdul-Halim, R., Fernando, M. et al. MR imaging features of spindle cell lipoma. Skeletal Radiol 43, 191–196 (2014). https://doi.org/10.1007/s00256-013-1765-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-013-1765-6