
Abstract
The goal of this study was to investigate metabolic risk factors in pediatric stone formers in an emerging economy. A prospective, data collection enrolled 250 children age <1–15 years at our center. Risk factors were evaluated by gender and in age groups <1–5, 6–10 and 11–15 years. Patients were evaluated for demographics, blood and 24 h urine for calcium, magnesium, phosphate, uric acid, electrolytes and additional protein, citrate, ammonia and oxalate in urine. All reported values were two sided and statistical significance was considered at p value ≤0.05. The mean age at diagnosis was 7.50 ± 3.56 years with a male to female ratio of 1.84:1. A family history of urolithiasis was found in 41 (16.4 %), urinary tract infection in 18 (7 %) and chronic diarrhea in 75 (30 %). Hypercalcemia was seen in 37 (14.8 %), hyperuricemia in 23 (9.2 %) and hyperphosphatemia in 6 (2.4 %). Urinary metabolic abnormalities were identified in 248 (98 %) of the cases. Hypocitraturia was found in 207 (82.8 %), hyperoxaluria in 62 (26.4 %), hyperuricosuria in 82 (32.8 %), hypercalciuria in 51 (20.4 %), hyperphosphaturia in 46 (18.4 %), hyperammonuria in 10 (4 %), hypocalciuria in 82 (32.8 %), and hypovolemia in 73 (29.2 %). Risk factors were similar between genders except higher rates of hyponatriuria, hypophosphaturia, and hypocalciuria in females. Hyperuricosuria, hyponatriuria, and hypovolemia were highest in 1–5 years (52, 49, 49 %) as compared to (18, 21, 12 %) those in 11–15 years (p < 0.001), respectively. This study shows that careful metabolic analysis can identify risk factors in 98 % of the children where appropriate metaphylaxis can be undertaken both for treatment and prevention of recurrence.


Similar content being viewed by others

References
Trinchieri A (2008) Epidemiology of urolithiasis: an update. Clin Cases Miner Bone Metab 5(2):101–106
Karsli O, Izol V, Aridogan IA, Borekoglu A, Satar N (2013) Metabolic risk factors and the effect of metaphylaxis in pediatric stone disease with hypocitraturia. Urolithiasis 41(1):9–13. doi:10.1007/s00240-012-0539-2
Hussain M, Rizvi SA, Askari H, Sultan G, Lal M, Ali B et al (2009) Management of stone disease: 17 years experience of a stone clinic in a developing country. J Pak Med Assoc 59(12):843–846
Rizvi SA, Naqvi SA, Hussain Z, Hashmi A, Hussain M, Zafar MN et al (2002) Pediatric urolithiasis: developing nation perspectives. J Urol 168(4 Pt 1):1522–1525
Rizvi SA, Sultan S, Zafar MN, Ahmed B, Faiq SM, Hossain KZ et al (2007) Evaluation of children with urolithiasis. Indian J Urol 23(4):420–427
Rizvi SA, Naqvi SA, Hussain Z, Hashmi A, Hussain M, Zafar MN et al (2002) The management of stone disease. BJU Int 89(1):62–68
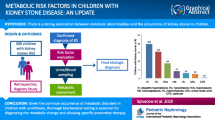
Spivacow FR, Negri AL, del Valle EE, Calviño I, Fradinger E, Zanchetta JR (2008) Metabolic risk factors in children with kidney stone disease. Pediatr Nephrol 23(7):1129–1133
Kliegman RM, Behrman RE, Schor NF, Stanton BF et al (2011) Nelson Textbook of Pediatrics. 19th edn. Elsevier/Saunders, London. p 1864
Hesse A, Tiselius HG, Siener R, Hoppe B (2009) Urinary stones diagnosis, treatment and prevention of recurrence, 3rd edn. Karger, London p, pp 44–166
Alpay H, Ozen A, Gokce I, Biyikli N (2009) Clinical and metabolic features of urolithiasis and microlithiasis in children. Pediatr Nephrol 24(11):2203–2209
Wu W, Yang D, Tiselius HG, Ou L, Liang Y, Zhu H, Li S, Zeng G (2014) The characteristics of the stone and urine composition in Chinese stone formers: primary report of a single-center results. Urology 83(4):732–737
Naseri M, Varasteh AR, Alamdaran SA (2010) Metabolic factors associated with urinary calculi in children. Iran J Kidney Dis 4(1):32–38
Le JD, Eisner BH, Tseng TY, Chi T, Stoller ML (2011) Laterality of nephrocalcinosis in kidney stone formers with severe hypocitraturia. BJU Int 107(1):106–110
Kurtz MP, Eisner BH (2011) Dietary therapy for patients with hypocitraturic nephrolithiasis. Nat Rev Urol 8(3):146–152
Tekin A, Tekgul S, Atsu N, Sahin A, Ozen H, Bakkaloglu M (2000) A study of the etiology of idiopathic calcium urolithiasis in children: hypocitraturia is the most important risk factor. J Urol 164:162–165
Sarica K (2006) Pediatric urolithiasis: etiology, specific pathogenesis and medical treatment. Urol Res 34(2):96–101
MacDougall L, Taheri S, Crofton P (2010) Biochemical risk factors for stone formation in a Scottish paediatric hospital population. Ann Clin Biochem 47(Pt 2):125–130
Borghi L, Meschi T, Amato F, Briganti A, Novarini A, Giannini A (1996) Urinary volume, water and recurrences in idiopathic calcium nephrolithiasis: a 5-year randomized prospective study. J Urol 155(3):839–843
Lal B, Paryani JP, Memon SU (2015) Childhood bladder stones-an endemic disease of developing countries. J Ayub Med Coll Abbottabad 27(1):17–21
Novak TE, Lakshmanan Y, Trock BJ, Gearhart JP, Matlaga BR (2009) Sex prevalence of pediatric kidney stone disease in the United States: an epidemiologic investigation. Urology 74(1):104–107
Koyuncu H, Yencilek F, Erturhan S, Eryildirım B, Sarica K (2011) Clinical course of pediatric urolithiasis: follow-up data in a long-term basis. Int Urol Nephrol 43(1):7–13
Kalorin CM, Zabiniski A, Okpareke I, White M, Kogan BA (2009) Pediatric urinary stone disease-does age matter? JUrol. 181:2267–2271
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Imran, K., Zafar, M.N., Ozair, U. et al. Metabolic risk factors in pediatric stone formers: a report from an emerging economy. Urolithiasis 45, 379–386 (2017). https://doi.org/10.1007/s00240-016-0922-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00240-016-0922-5