
Abstract
Purpose
The aims of this study were to describe combinations of beta-blockers (BB), renin-angiotensin system (RAS) blockers, and mineralocorticoid receptor antagonist (MRA) prescriptions and their trajectories in heart failure with preserved ejection fraction (HFpEF) patients, and to assess their effect on the three-year all-cause and cardiovascular (CV)-mortality.
Methods
We used data from the EPICAL2 cohort of 689 hospitalized HFpEF patients. Medication prescriptions were collected at hospital discharge and at 6, 12, and 24 months after discharge. A multi-trajectory approach was used to conjointly model groups of individuals following similar trajectories over medications prescriptions. We used Cox and Fine‐Gray models, to evaluate respectively the associations between 3-year all‐cause mortality and CV-mortality and the trajectory groups.
Results
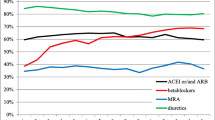
Multi-trajectory modelling revealed five distinct trajectory groups: group1 (N = 232, 33.6%) stable ACEI/ARB and BB prescriptions, group 2 (N = 199, 28.8%) stable ACEI/ARB prescription, group 3 (N = 133, 19.3%) stable BB prescriptions, group 4 (N = 78, 11.3%) stable prescriptions of none of the medications, and group 5 (N = 47, 6.8%) stable ACEI/ARB, BB, and MRA prescriptions. As compared to the group 4 of patients receiving none of the three medications, patients receiving a stable prescription of one or a combination of two or the three medications over 2 years) had a lower overall mortality over 3-year follow-up, i.e., group 1 (HR = 0.5, 95% CI 0.4–0.8), group 2 (HR = 0.6, 95% CI:0.4–0.8), group 3 (HR = 0.5, 95% CI:0.4–0.7), and group 5 (HR = 0.5, 95% CI:0.3–0.9). However, none of these trajectory groups was associated with a lower CV-mortality over 3 years.
Conclusion
In an unselected population-based sample of HFpEF patients, the long-term stable use of the combination ACEI/ARB and BB, BB exclusively, ACEI/ARB exclusively, or the combination ACEI/ARB and BB and MRAs was associated with reduced three-year all-cause mortality.




Similar content being viewed by others


Availability of data and material
Data archiving is not mandated but data will be made available on reasonable request.
Abbreviations
- ACEI:
-
Angiotensin-converting enzyme inhibitor
- ARB:
-
Angiotensin II receptor blockers
- BB:
-
Beta-blockers
- BIC:
-
Bayesian information criterion
- BMI:
-
Body mass index
- COPD:
-
Chronic obstructive pulmonary disease
- CKD:
-
Chronic kidney disease
- CV:
-
Cardiovascular
- EPICAL2:
-
Epidemiologie et Pronostic de l’Insuffisance Cardiaque Aigue en Lorraine
- GBTM:
-
Group-based trajectory modelling
- HFpEF:
-
Heart failure with preserved ejection fraction
- HFrEF:
-
Heart failure and reduced ejection fraction
- MAR:
-
Missing at random
- MCAR:
-
Missing completely at random
- MRAs:
-
Mineralocorticoid receptor antagonists
- NYHA:
-
New York Heart Association
- RAS:
-
Renin-angiotensin system
- RCT:
-
Randomized controlled trials
References
Sharma K, Kass D (2014) Heart failure with preserved ejection fraction. Circ Res 115(1):79–96
van Riet EES, Hoes AW, Wagenaar KP, Limburg A, Landman MAJ, Rutten FH (2016) Epidemiology of heart failure: the prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur J Heart Fail 18(3):242–252
Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM (2006) Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 355(3):251–259
Carson PE, Anand IS, Win S, Rector T, Haass M, Lopez-Sendon J et al (2015) The hospitalization burden and post-hospitalization mortality risk in heart failure with preserved ejection fraction: results from the I-PRESERVE trial (Irbesartan in Heart Failure and Preserved Ejection Fraction). JACC: Heart Failure 3(6):429–441
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS et al (2016) 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur J Heart Fail 18(8):891–975
van Veldhuisen DJ, Cohen-Solal A, Böhm M, Anker SD, Babalis D, Roughton M et al (2009) Beta-blockade with nebivolol in elderly heart failure patients with impaired and preserved left ventricular ejection fraction: Data From SENIORS (Study of Effects of Nebivolol Intervention on Outcomes and Rehospitalization in Seniors With Heart Failure). J Am Coll Cardiol 53(23):2150–2158
Cleland JGF, Tendera M, Adamus J, Freemantle N, Polonski L, Taylor J et al (2006) The perindopril in elderly people with chronic heart failure (PEP-CHF) study. Eur Heart J 27(19):2338–2345
Massie BM, Carson PE, McMurray JJ, Komajda M, McKelvie R, Zile MR et al (2008) Irbesartan in patients with heart failure and preserved ejection fraction. N Engl J Med 359(23):2456–2467
Yusuf S, Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJV et al (2003) Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARM-Preserved Trial. Lancet 362(9386):777–781
Pitt B, Pfeffer MA, Assmann SF, Boineau R, Anand IS, Claggett B et al (2014) Spironolactone for heart failure with preserved ejection fraction. N Engl J Med 370(15):1383–1392
Steinberg BA, Zhao X, Heidenreich PA, Peterson ED, Bhatt DL, Cannon CP et al (2012) Trends in patients hospitalized with heart failure and preserved left ventricular ejection fraction: prevalence, therapies, and outcomes. Circulation 126(1):65–75
Cohen Solal A, Leurs I, Assyag P, Beauvais F, Clerson P, Contre C et al (2012) Optimization of heart FailUre medical Treatment after hospital discharge according to left ventricUlaR Ejection fraction: The FUTURE survey. Arch Cardiovasc Dis 105(6):355–365
Goldberg RJ, Gurwitz JH, Saczynski JS, Hsu G, McManus DD, Magid DJ et al (2013) Comparison of medication practices in patients with heart failure and preserved versus those with reduced ejection fraction (from the Cardiovascular Research Network [CVRN]). Am J Cardiol 111(9):1324–1329
Yancy CW, Lopatin M, Stevenson LW, De Marco T, Fonarow GC (2006) Clinical presentation, management, and in-hospital outcomes of patients admitted with acute decompensated heart failure with preserved systolic function: a report from the Acute Decompensated Heart Failure National Registry (ADHERE) Database. J Am Coll Cardiol 47(1):76–84
Chioncel O, Lainscak M, Seferovic PM, Anker SD, Crespo-Leiro MG, Harjola V-P et al (2017) Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: an analysis of the ESC Heart Failure Long-Term Registry. Eur J Heart Fail 19(12):1574–1585
Maggioni AP, Anker SD, Dahlström U, Filippatos G, Ponikowski P, Zannad F et al (2013) Are hospitalized or ambulatory patients with heart failure treated in accordance with European Society of Cardiology guidelines? Evidence from 12,440 patients of the ESC Heart Failure Long-Term Registry. Eur J Heart Fail 15(10):1173–1184
Lund LH, Benson L, Dahlström U, Edner M (2012) Association between use of renin-angiotensin system antagonists and mortality in patients with heart failure and preserved ejection fraction. JAMA 308(20):2108–2117
Agarwal V, Briasoulis A, Messerli FH (2013) Effects of renin-angiotensin system blockade on mortality and hospitalization in heart failure with preserved ejection fraction. Heart Fail Rev 18(4):429–437
Fukuta H, Goto T, Wakami K, Ohte N (2017) The effect of beta-blockers on mortality in heart failure with preserved ejection fraction: a meta-analysis of observational cohort and randomized controlled studies. Int J Cardiol 1(228):4–10
Bitar S, Agrinier N, Alla F, Rossignol P, Mebazaa A, Thilly N (2019) Adherence to ESC guideline-recommended medications over a 36-month follow-up period after hospitalization for heart failure: results from the EPICAL2 cohort study. Pharmacoepidemiol Drug Saf 28(11):1489–1500
Busson A, Thilly N, Laborde-Castérot H, Alla F, Messikh Z, Clerc-Urmes I et al (2018) Effectiveness of guideline-consistent heart failure drug prescriptions at hospital discharge on 1-year mortality: results from the EPICAL2 cohort study. Eur J Intern Med 1(51):53–60
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40(5):373–383
Jones BL, Nagin DS, Roeder K (2001) A SAS procedure based on mixture models for estimating developmental trajectories. Sociol Methods Res 29(3):374–393
Nagin DS, Jones BL, Passos VL, Tremblay RE (2018) Group-based multi-trajectory modeling. Stat Methods Med Res 27(7):2015–2023
Nagin DS, Odgers CL (2010) Group-based trajectory modeling in clinical research. Annu Rev Clin Psychol 6:109–138
Schwartz T, Chen Q, Duan N (2011) Studying missing data patterns using a SAS® Macro. 4:339
Suissa S (2008) Immortal time bias in pharmaco-epidemiology. Am J Epidemiol 167(4):492–499
Agarwal P, Moshier E, Ru M, Ohri N, Ennis R, Rosenzweig K, et al (2018) Immortal time bias in observational studies of time-to-event outcomes. Cancer Control [Internet]. [cited 2019 Nov 8];25(1). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6053873/
Neefs J, van den Berg NWE, Limpens J, Berger WR, Boekholdt SM, Sanders P et al (2017) Aldosterone pathway blockade to prevent atrial fibrillation: a systematic review and meta-analysis. Int J Cardiol 15(231):155–161
Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJV, Ponikowski P, Poole-Wilson PA et al (2008) ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the diagnosis and treatment of acute and chronic heart failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur J Heart Fail 10(10):933–989
Hernandez AF, Hammill BG, O’Connor CM, Schulman KA, Curtis LH, Fonarow GC (2009) Clinical effectiveness of beta-blockers in heart failure: findings from the OPTIMIZE-HF (Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure) Registry. J Am Coll Cardiol 53(2):184–192
Peltier M, Houpe D, Cohen-Solal A, Béguin M, Levy F, Tribouilloy C (2007) Treatment practices in heart failure with preserved left ventricular ejection fraction: a prospective observational study. Int J Cardiol 118(3):363–369
Bavishi C, Chatterjee S, Ather S, Patel D, Messerli FH (2015) Beta-blockers in heart failure with preserved ejection fraction: a meta-analysis. Heart Fail Rev 20(2):193–201
Khan MS, Fonarow GC, Khan H, Greene SJ, Anker SD, Gheorghiade M et al (2017) Renin-angiotensin blockade in heart failure with preserved ejection fraction: a systematic review and meta-analysis. ESC Heart Fail 4(4):402–408
Martin N, Manoharan K, Thomas J, Davies C, Lumbers RT (2018) Beta-blockers and inhibitors of the renin-angiotensin aldosterone system for chronic heart failure with preserved ejection fraction. Cochrane Database Syst Rev 28(6):CD012721
Zheng SL, Chan FT, Nabeebaccus AA, Shah AM, McDonagh T, Okonko DO et al (2018) Drug treatment effects on outcomes in heart failure with preserved ejection fraction: a systematic review and meta-analysis. Heart 104(5):407–415
Tsujimoto T, Kajio H (2018) Beta-blocker use and cardiovascular event risk in patients with heart failure with preserved ejection fraction. Sci Rep [Internet]. [cited 2020 Apr 23];8. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6015007/
Triposkiadis F, Karayannis G, Giamouzis G, Skoularigis J, Louridas G, Butler J (2009) The sympathetic nervous system in heart failure physiology, pathophysiology, and clinical implications. J Am Coll Cardiol 54(19):1747–1762
Tschöpe C, Birner C, Böhm M, Bruder O, Frantz S, Luchner A et al (2018) Heart failure with preserved ejection fraction: current management and future strategies: expert opinion on the behalf of the Nucleus of the “Heart Failure Working Group” of the German Society of Cardiology (DKG). Clin Res Cardiol 107(1):1–19
Senni M, Paulus WJ, Gavazzi A, Fraser AG, Díez J, Solomon SD et al (2014) New strategies for heart failure with preserved ejection fraction: the importance of targeted therapies for heart failure phenotypes. Eur Heart J 35(40):2797–2815
Nanayakkara S, Kaye DM (2015) Management of heart failure with preserved ejection fraction: a review. Clin Ther 37(10):2186–2198
Costantino G, Rusconi AM, Duca PG, Guzzetti S, Bossi I, Del Medico M et al (2009) Eligibility criteria in heart failure randomized controlled trials: a gap between evidence and clinical practice. Intern Emerg Med 4(2):117–122
Patel HC, Hayward C, Dungu JN, Papadopoulou S, Saidmeerasah A, Ray R et al (2017) Assessing the eligibility criteria in phase III randomized controlled trials of drug therapy in heart failure with preserved ejection fraction: the critical play-off between a “pure” patient phenotype and the generalizability of trial findings. J Card Fail 23(7):517–524
Girerd N, Seronde M-F, Coiro S, Chouihed T, Bilbault P, Braun F et al (2018) Integrative assessment of congestion in heart failure throughout the patient journey. JACC: Heart Failure 6(4):273–285
Massari F, Scicchitano P, Iacoviello M, Passantino A, Guida P, Sanasi M et al (2020) Multiparametric approach to congestion for predicting long-term survival in heart failure. J Cardiol 75(1):47–52
Acknowledgements
The authors thank all physicians from the 21 participating centers in the EPICAL2 clinical cohort study (Hôpitaux de Brabois et Hôpital Central, CHU Nancy; CH Luneville; Espace chirurgical Ambroise Paré Nancy; CH Alpha Santé Mont-Saint-Martin; CH Pont-à-Mousson; CH Saint-Nicolas Verdun; Hôpital Bon-Secours CHR Metz; CH Freyming Merlebach; Hôpital Sainte-Blandine Metz; Hôpital Bel Air CHR Thionville; CH Marie-Madeleine Forbach; Hôpital Alpha Santé Hayange; CH Saint-Nicolas Sarrebourg; Hôpital Lemire SaintAvold; Hôpital des Armées Legouest Metz; Clinique Claude Bernard Metz; CH Saint-Charles Saint-Dié; CH Jean Monnet Epinal; CH Neufchateau; CH Vittel). We would also like to thank all participants and patients of EPICAL2.
Funding
The EPICAL2 cohort study was funded as part of the 2009 National Hospital Program of Clinical Research (PHRC 2009) of the French Ministry of Health and by the RHU Fight-HF, a public grant overseen by the French National Research Agency (ANR) as part of the second “Investissements d’Avenir” program (reference: ANR-15-RHUS-0004).
Author information
Authors and Affiliations
Contributions
Nelly Agrinier, and Nathalie Thilly contributed to conception and design of the study, data acquisition and interpretation of results, and critically revised the manuscript; Sarah Bitar contributed to analysis and interpretation, and drafted manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Bitar, S., Thilly, N. & Agrinier, N. Prognostic association of medication trajectories with 3-year mortality in heart failure and preserved ejection fraction: findings from the EPICAL2 cohort study. Eur J Clin Pharmacol 77, 1569–1581 (2021). https://doi.org/10.1007/s00228-021-03153-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-021-03153-6