
Abstract
Objective
Genetic polymorphisms of arylamine N-acetyltransferase 2 (NAT2) result in large interindividual differences in the plasma concentration of isoniazid (INH). We hypothesized that the internationally recommended dosage should be increased for patients with two active NAT2 alleles (RA type) in order to achieve appropriate antituberculous efficiency; however, the pharmacokinetic effects of the dose increase have not been fully addressed. To estimate an optimal dosage for RA-type patients, we conducted a dose escalation study in healthy male volunteers carrying NAT2*4/*4.
Methods
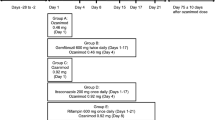
Oral doses of 300 mg, 600 mg, and 900 mg of INH were administered to eight RA-type subjects, whereas 300 mg was administered to eight IA-type subjects with one active allele (NAT2*4). The pharmacokinetic parameters were estimated from plasma INH concentrations for 24 h postdose.
Results
The ratio of the mean area under the plasma-concentration time curve (AUC) was not proportional to the doses (1:2.6:5.0 for 300:600:900-mg dose) in parallel to the plasma concentration at 1 h (C1) and 2 h (C2) after administration. Compared with the IA-type group given 300 mg, the RA-type group had lower pharmacokinetic parameters at 300 mg (AUC, 66%; C1, 72%; C2, 61%), but higher parameters at 600 mg (AUC, 175%; C1, 196%; C2, 170%). Plasma concentrations of the IA-type group were within the therapeutic range. An optimal INH dose was calculated as 430 mg (7.2 mg/kg) for RA-type subjects to obtain an AUC comparable with that in IA-type subjects dosed with 300 mg.
Conclusion
In RA-type subjects, the pharmacokinetic parameters appeared to lack linearity with the increased dose of INH. We propose that the proper daily dose for RA-type patients is 1.5-times higher than that currently recommended.

Similar content being viewed by others

References
Blumberg HM, Burman WJ, Chaisson RE, Daley CL, Etkind SC, Friedman LN, Fujiwara P, Grzemska M, Hopewell PC, Iseman MD, Jasmer RM, Koppaka V, Menzies RI, O’Brien RJ, Reves RR, Reichman LB, Simone PM, Starke JR, Vernon AA (2003) American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis. Am J Respir Crit Care Med 167:603–662
Yee D, Valiquette C, Pelletier M, Parisien I, Rocher I, Menzies D (2003) Incidence of serious side effects from first-line antituberculosis drugs among patients treated for active tuberculosis. Am J Respir Crit Care Med 167:1472–1477
Deguchi T, Mashimo M, Suzuki T (1990) Correlation between acetylator phenotypes and genotypes of polymorphic arylamine N-acetyltransferase in human liver. J Biol Chem 265:12757–12760
Cascorbi I, Drakoulis N, Brockmoller J, Maurer A, Sperling K, Roots I (1995) Arylamine N-acetyltransferase (NAT2) mutations and their allelic linkage in unrelated Caucasian individuals: correlation with phenotypic activity. Am J Hum Genet 57:581–592
Butcher NJ, Boukouvala S, Sim E, Minchin RF (2002) Pharmacogenetics of the arylamine N-acetyltransferases. Pharmacogenomics J 2:30–42
Parkin DP, Vandenplas S, Botha FJ, Vandenplas ML, Seifart HI, van Helden PD, van der Walt BJ, Donald PR, van Jaarsveld PP (1997) Trimodality of isoniazid elimination: phenotype and genotype in patients with tuberculosis. Am J Respir Crit Care Med 155:1717–1722
Ohno M, Yamaguchi I, Yamamoto I, Fukuda T, Yokota S, Maekura R, Ito M, Yamamoto Y, Ogura T, Maeda K, Komuta K, Igarashi T, Azuma J (2000) Slow N-acetyltransferase 2 genotype affects the incidence of isoniazid and rifampicin-induced hepatotoxicity. Int J Tuberc Lung Dis 4:256–261
Huang YS, Chern HD, Su WJ, Wu JC, Lai SL, Yang SY, Chang FY, Lee SD (2002) Polymorphism of the N-acetyltransferase 2 gene as a susceptibility risk factor for antituberculosis drug-induced hepatitis. Hepatology 35:883–889
Shimizu Y, Dobashi K, Mita Y, Endou K, Moriya S, Osano K, Koike Y, Higuchi S, Yabe S, Utsugi M, Ishizuka T, Hisada T, Nakazawa T, Mori M (2006) DNA microarray genotyping of N-acetyltransferase 2 polymorphism using carbodiimide as the linker for assessment of isoniazid hepatotoxicity. Tuberculosis (Edinb) 86:374–381
Kimerling ME, Phillips P, Patterson P, Hall M, Robinson CA, Dunlap NE (1998) Low serum antimycobacterial drug levels in non-HIV-infected tuberculosis patients. Chest 113:1178–1183
Weiner M, Burman W, Vernon A, Benator D, Peloquin CA, Khan A, Weis S, King B, Shah N, Hodge T (2003) Low isoniazid concentrations and outcome of tuberculosis treatment with once-weekly isoniazid and rifapentine. Am J Respir Crit Care Med 167:1341–1347
Ozawa S, Katoh T, Inatomi H, Imai H, Kuroda Y, Ichiba M, Ohno Y (2002) Association of genotypes of carcinogen-activating enzymes, phenol sulfotransferase SULT1A1 (ST1A3) and arylamine N-acetyltransferase NAT2, with urothelial cancer in a Japanese population. Int J Cancer 102:418–421
Peloquin CA, Jaresko GS, Yong CL, Keung AC, Bulpitt AE, Jelliffe RW (1997) Population pharmacokinetic modeling of isoniazid, rifampin, and pyrazinamide. Antimicrob Agents Chemother 41:2670–2679
Brockmoller J, Cascorbi I, Kerb R, Roots I (1996) Combined analysis of inherited polymorphisms in arylamine N-acetyltransferase 2, glutathione S-transferases M1 and T1, microsomal epoxide hydrolase, and cytochrome P450 enzymes as modulators of bladder cancer risk. Cancer Res 56:3915–3925
Peloquin CA (2002) Therapeutic drug monitoring in the treatment of tuberculosis. Drugs 62:2169–2183
Kinzig-Schippers M, Tomalik-Scharte D, Jetter A, Scheidel B, Jakob V, Rodamer M, Cascorbi I, Doroshyenko O, Sorgel F, Fuhr U (2005) Should we use N-acetyltransferase type 2 genotyping to personalize isoniazid doses? Antimicrob Agents Chemother 49:1733–1738
Donald PR, Sirgel FA, Venter A, Parkin DP, Seifart HI, van de Wal BW, Werely C, van Helden PD, Maritz JS (2004) The influence of human N-acetyltransferase genotype on the early bactericidal activity of isoniazid. Clin Infect Dis 39:1425–1430
Ohno M, Kubota R, Yasunaga M, Yokota S, Azuma J (2004) Population pharmacokinetics and pharmacogenetics trial of isoniazid. Clin Exp Pharmacol Physiol 31(Suppl):A138
Kubota R, Ohno M, Yasunaga M, Yokota S, Maekura R, Azuma J (2005) Tentative treatments for tuberculosis based on N-acetyltransferase gene polymorphism. Jpn J Therapeutic Drug Monitoring 22:336–340
Hickman D, Pope J, Patil SD, Fakis G, Smelt V, Stanley LA, Payton M, Unadkat JD, Sim E (1998) Expression of arylamine N-acetyltransferase in human intestine. Gut 42:402–409
Acknowledgements
This study was supported in part by grants from Research on Health Sciences Focusing on Drug Innovation, The Japan Health Sciences Foundation (KH31036), by the Pfizer Health Research Foundation, by Grant-in-Aid for Scientific Research (19390042), and Takeda Science Foundation. It was also supported in part by grants from Health and Labour Sciences Research Grant, by the Japanese Research Foundation for Clinical Pharmacology, by the Suzuken Memorial Foundation. We are grateful to Dr. Y. Fujio (Osaka University) for his critical review of the manuscript. Special acknowledgements go to MSc. M. Watanabe for her development of the INH determination method by HPLC. We thank Dr. T. Fukuda, MSc. M. Furutsuka, MSc. S. Nakayama, and MSc. T. Tanabe, our colleagues, for their help. We also thank Mr. M. Takebe and Dr. C. Iwata for providing the opportunity for the clinical trial. The technical assistance from all the staff of the Kitasato Institute is appreciated.
Conflict of interest statement
The study received no support from the pharmaceutical industry. None of the authors has any conflict of interest regarding this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kubota, R., Ohno, M., Hasunuma, T. et al. Dose-escalation study of isoniazid in healthy volunteers with the rapid acetylator genotype of arylamine N-acetyltransferase 2. Eur J Clin Pharmacol 63, 927–933 (2007). https://doi.org/10.1007/s00228-007-0333-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-007-0333-1