
Abstract
Summary
Our imminent model was less sensitive but more selective than FRAX® in the choice of treatment to prevent imminent fractures. This new model decreased NNT by 30%, which could reduce the treatment costs. In the Belgian FRISBEE cohort, the effect of recency further decreased the selectivity of FRAX®.
Purpose
We analyzed the selection for treatment of patients at high risk of fracture by the Belgian FRISBEE imminent model and the FRAX® tool.
Methods
We identified in the FRISBEE cohort subjects who sustained an incident MOF (mean age 76.5 ± 6.8 years). We calculated their estimated 10-year risk of fracture using FRAX® before and after adjustment for recency and the 2-year probability of fracture using the FRISBEE model.
Results
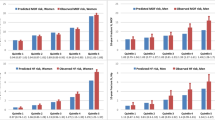
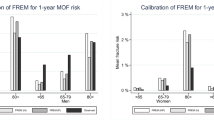
After 6.8 years of follow-up, we validated 480 incident and 54 imminent MOFs. Of the subjects who had an imminent fracture, 94.0% had a fracture risk estimated above 20% by the FRAX® before correction for recency and 98.1% after adjustment, with a specificity of 20.2% and 5.9%, respectively. The sensitivity and specificity of the FRISBEE model at 2 years were 72.2% and 55.4%, respectively, for a threshold of 10%.
For these thresholds, 47.3% of the patients were identified at high risk in both models before the correction, and 17.2% of them had an imminent MOF. The adjustment for recency did not change this selection. Before the correction, 34.2% of patients were selected for treatment by FRAX® only, and 18.8% would have had an imminent MOF. This percentage increased to 47% after the adjustment for recency, but only 6% of those would suffer a MOF within 2 years.
Conclusion
In our Belgian FRISBEE cohort, the imminent model was less sensitive but more selective in the selection of subjects in whom an imminent fracture should be prevented, resulting in a lower NNT. The correction for recency in this elderly population further decreased the selectivity of FRAX®. These data should be validated in additional cohorts before using them in everyday practice.


Similar content being viewed by others

References
Kanis JA, Harvey NC et al (2020) A decade of FRAX: how has it changed the management of osteoporosis? Aging Clin Exp Res 32:187–196
McCloskey EV, Borgstrom F, Cooper C et al (2021) Short time horizons for fracture prediction tools: time for a rethink. Osteoporos Int 32(6):1019–1025
Iconaru L, Baleanu F, Charles A et al (2021) Which treatment to prevent an imminent fracture? Bone Rep 15:101105
Kanis JA, Johansson H, Harvey NC et al (2020) Adjusting conventional FRAX estimates of fracture probability according to the recency of sentinel fractures. Osteoporos Int 31:1817–1828
Kanis J, Johansson H, Harvey N et al (2021) The use of 2-, 5-, and 10-year probabilities to characterize fracture risk after a recent sentinel fracture. Osteoporos Int 32:47–54
Iconaru L, Charles A, Baleanu F et al (2023) The effect of fracture recency on observed 5-year fracture probability: a study based on the FRISBEE cohort. Bone Rep 18:101660
Iconaru L, Charles A, Baleanu F et al (2021) Prediction of an imminent fracture after an index fracture – models derived from the FRISBEE cohort. J Bone Miner Res 37(1):59–67
Iconaru L, Moreau M, Baleanu F, et. (2021) Risk factors for imminent fractures: a substudy of the FRISBEE cohort. Osteoporos Int 32(6):1093–1101
Baleanu F, Iconaru L, Charles A et al (2021) Independent external validation of FRAX® and Garvan fracture risk calculators: a substudy of the FRISBEE cohort. JBMR Plus 5(9):e10532
Leslie WD, Lix LM, Johansson H et al (2010) Independent clinical validation of a Canadian FRAX tool: fracture prediction and model calibration. J Bone Miner Res 25(11):2350–2358
Bolland MJ, Siu AT, Mason BH et al (2011) Evaluation of the FRAX and Garvan fracture risk calculators in older women. J Bone Miner Res 26(2):420–427
Koo TK, Li MY (2016) A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med 15(2):155–163
Cappelle SI, Ramon I, Dekelver C et al (2017) Distribution of clinical risk factors for fracture in a Brussels cohort of postmenopausal women: the FRISBEE study and comparison with other major cohort studies. Maturitas 106:1–7
Baleanu F, Moreau M, Kinnard V et al (2020) What is the validity of self-reported fractures? Bone Rep 1(12):100256
Baleanu F, Moreau M, Kinnard V et al (2020) Underevaluation of fractures by self-report: an analysis from the FRISBEE cohort. Arch Osteoporos 15(1):61
Johansson H, Kanis JA, McCloskey OA et al (2011) A FRAX model for the assessment of fracture probability in Belgium. Osteoporos Int 22:453–461
Mugisha A, Bergmann P, Kinnard V et al (2021) MOF/Hip Fracture Ratio in a Belgian Cohort of Post-menopausal Women (FRISBEE): potential impact on the FRAX® Score. Calcif Tissue Int 109(6):600–604
Tosteson ANA, Melton LJ, Dawson-Hughes B et al (2008) Cost-effective osteoporosis treatment thresholds: the United States perspective. Osteoporos Int 19(4):437–447
Sanchez-Rodriguez D, Bergmann P, Body JJ et al (2020) The Belgian Bone Club 2020 guidelines for the management of osteoporosis in postmenopausal women. Maturitas 139:69–89
Leslie WD, Morin SN, Lix LM et al (2022) The effect of fracture recency on observed 10-year fracture probability: a registry-based cohort study. J Bone Miner Res 37(5):848–855
Hernlund E, Svedbom A, Ivergård M et al (2013) Osteoporosis in the European Union: medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch Osteoporos 8:136
Crandall CJ, Hovey KM, Cauley JA et al (2015) Wrist fracture and risk of subsequent fracture: findings from the Women’s Health Initiative Study. J Bone Miner Res 30(11):2086–2095
Shauver MJ, Zhong L, Chung KC et al (2015) Mortality after distal radial fractures in the Medicare population. J Hand Surg Eur 40(8):805–811
Borgen TT, Bjørnerem A, Solberg LB et al (2019) Post-fracture risk assessment: target the centrally sited fractures first! A substudy of NoFRACT. J Bone Miner Res 34(11):2036–2044
Acknowledgements
The FRISBEE study is supported by CHU Brugmann and IRIS-Recherche.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary file 1
Supplementary Table 1. Distribution of incident fractures in two models: imminent MOFs model and recalculated FRAX® with correction for recency. Supplementary Table 2. Distribution of imminent fractures in two models: imminent MOFs model and recalculated FRAX® with correction for recency
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Iconaru, L., Charles, A., Baleanu, F. et al. Selection for treatment of patients at high risk of fracture by the short versus long term prediction models — data from the Belgian FRISBEE cohort. Osteoporos Int 34, 1119–1125 (2023). https://doi.org/10.1007/s00198-023-06737-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-023-06737-3