
Abstract
Summary
The Fine-Gray method is often used instead of Cox regression to account for competing risks of death in time-to-event analyses for non-fatal outcomes. A series of examples using well-known risk factors of hip fracture in an older cohort with substantial competing mortality demonstrates that the Fine-Gray approach can yield estimates that implausibly contradict long-established associations, while Cox regression preserves them. Cox regression is generally preferred for risk factor-outcome associations even in the presence of competing risk of death.
Introduction
Factors like age, sex, and race are associated not only with risk of hip fracture but also with mortality. Substantial misunderstanding remains regarding the appropriate statistical approach to account for the competing risk of mortality.
Methods
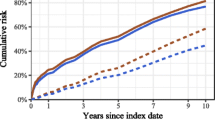
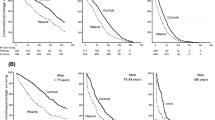
In the Cardiovascular Health Study, an ongoing cohort study of 5888 older adults, we followed participants for incident hip fracture from their 1992–1993 visit through June 2014. We contrasted the conventional cause-specific Cox analysis, which censors individuals at the time of death, with the Fine-Gray (FG) approach, which extends participant follow-up even after death, to estimate the association of well-established demographic and clinical factors with incident hip fracture.
Results
For age, current smoking and sex, Cox and FG methods yielded directionally concordant but quantitatively different strengths of association. For example, the Cox hazard ratio (HR) for a 5-year increment in age was 1.74 (95% CI, 1.61–1.87), while the corresponding FG HR was 1.16 (1.09–1.24). In contrast, the FG approach estimated a stronger association of hip fracture with sex. The two approaches yielded nearly identical results for race. For diabetes and kidney function, the estimates were discordant in direction, and the FG HRs suggested effects that were in the opposite direction of well-understood and widely accepted associations.
Conclusions
Cause-specific Cox models provide appropriate estimates of hazard for non-fatal outcomes like hip fracture even in the presence of competing risk of mortality. The Cox approach estimates hazard in the population of individuals who have not yet had an incident hip fracture and remain alive, which is typically the group of clinical interest. The Fine-Gray method estimates hazard in a hypothetical population that can yield misleading inferences about risk factors in populations of clinical interest.
Similar content being viewed by others

References
Berry S, Ngo L, Samelson EJ, Kiel D (2010) Competing risk of death: an important consideration in studies of older adults. J Am Geriatr Soc 58(4):783–787
Fine JP, Gray RJ (1999) A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc 94(446):496–509
Austin PC, Fine JP (2017) Practical recommendations for reporting Fine-Gray model analyses for competing risk data. Stat Med 36:4391–4400
Austin PC, Lee DS, Fine JP (2016) Introduction to the analysis of survival data in the presence of competing risks. Circulation. 83:311–321
Latouche A, Allignol A, Beyersmann J, Labopin M, Fine JP (2013) A competing risks analysis should report results on all cause-specific hazards and cumulative incidence functions. J Clin Epidemiol 66(6):648–653
Szulc P, Blackwell T, Kiel DP, Schousboe JP, Cauley J, Hillier T et al (2015) Abdominal aortic calcification and risk of fracture among older women the SOF study. Bone. 81:16–23
Prez-Sez M, Prieto-Alhambra D, Barrios C, Crespo M, Redondo D, Nogus X et al (2015) Increased hip fracture and mortality in chronic kidney disease individuals: the importance of competing risks. Bone. 73:154–159
Basu U, Goodbrand J, Turdo ME, Donnan PT, McGilchrist M, Frost H et al (2016) Association between allopurinol use and hip fracture in older patients. Bone. 84:189–193
Cauley J, Cawthon P, Peters K, Cummings S, Ensrud K, Bauer D et al (2016) Risk factors for hip fracture in older men: the osteoporotic fractures in men study (MrOS). J Bone Miner Res 31(10):1810–1819
Cox D, Oakes D (1984) Analysis of survival data. Chapman and Hall
Cox DR (1972) Regression models and life-tables. J R Stat Soc Ser B Methodol 34(2):187–220
Wolbers M, Koller M, Stel VS, Jager K, Le ondre K, Heinze G (2014) Competing risks analyses: objectives and approaches. Eur Heart J 35:2936–2941
Ferreira-Gonzalez I, Permanyer-Miralda G, Busse JW, Bryant DM, Montori VM, Alonso-Coello P et al (2007) Methodologic discussions for using and interpreting composite endpoints are limited, but still identify major concerns. J Clin Epidemiol 60(7):651–657
Fried LP, Borhani NO, Enright P, Furberg CD, Gardin JM, Kronmal RA, Kuller LH, Manolio TA, Mittelmark MB, Newman A, O’Leary DH, Psaty B, Rautaharju P, Tracy RP, Weiler PG (1991) The cardiovascular health study: design and rationale. Ann Epidemiol 1(3):263–276
Wu Z-J, Zhao P, Liu B, Yuan Z-C (2016) Effect of cigarette smoking on risk of hip fracture in men: a meta-analysis of 14 prospective cohort studies. PLoS One 11(12):e0168990. https://doi.org/10.1371/journal.pone.0168990
Shen GS, Li Y, Zhao G, Zhou HB, Xie ZG, Xu W, Chen HN, Dong QR, Xu YJ (2015) Cigarette smoking and risk of hip fracture in women: a meta-analysis of prospective cohort studies. Injury. 46(7):1333–1340
Kanis JA, Johnell O, Oden A, Johansson H, De Laet C, Eisman JA et al (2005) Smoking and fracture risk: a meta-analysis. Osteoporos Int 16(2):155–162
Daya NR, Voskertchian A, Schneider ALC, Ballew S, McAdams Demarco M, Coresh J, Appel LJ, Grams ME (2016) Kidney function and fracture risk: the atherosclerosis risk in communities (ARIC) study. Am J Kidney Dis 67(2):218–226
Schneider ALC, Williams EK, Brancati FL, Blecker S, Coresh J, Selvin E (2013) Diabetes and risk of fracture-related hospitalization: the atherosclerosis risk in communities study. Diabetes Care 36(5):1153–1158. https://doi.org/10.2337/dc12-1168
Fan Y, Wei F, Lang Y, Liu Y (2016) Diabetes mellitus and risk of hip fractures: a meta-analysis. Osteoporos Int 27:219–228
R Development Core Team (2018) R: a language and environment for statistical computing. R Foundation for Statistical Computing: Vienna. ISBN 3-900051-07-0. http://www.R-project.org
Acknowledgments
A full list of principal CHS investigators and institutions can be found at CHS-NHLBI.org.
Funding
This research was supported by contracts HHSN268201200036C, HHSN268200800007C, HHSN268201800001C, N01HC55222, N01HC85079, N01HC85080, N01HC85081, N01HC85082, N01HC85083, and N01HC85086 and grants U01HL080295 and U01HL130114 from the National Heart, Lung, and Blood Institute (NHLBI), with additional contribution from the National Institute of Neurological Disorders and Stroke (NINDS). Additional support was provided by R01AG023629 from the National Institute on Aging (NIA).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Buzkova, P., Barzilay, J.I. & Mukamal, K.J. Assessing risk factors of non-fatal outcomes amid a competing risk of mortality: the example of hip fracture. Osteoporos Int 30, 2073–2078 (2019). https://doi.org/10.1007/s00198-019-05048-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-019-05048-w